






























































More Related Content
What's hot (20)
Similar to Peptic ulcer (20)


















Recently uploaded (20)




















Peptic ulcer
- 1. Benign Gastric and Duodenal Ulcers Dr.Sujith Mathew Jose PG in General Surgery Coimbatore Medical College Coimbatore
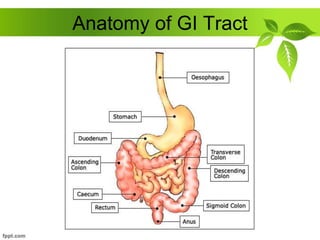
- 2. Anatomy of GI Tract
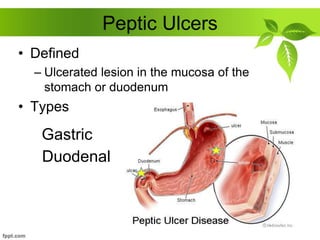
- 3. Peptic Ulcers • Defined – Ulcerated lesion in the mucosa of the stomach or duodenum • Types Gastric Duodenal
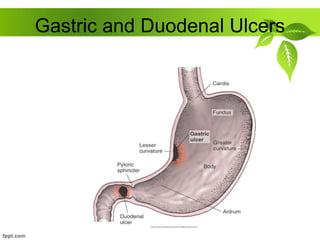
- 4. Gastric and Duodenal Ulcers
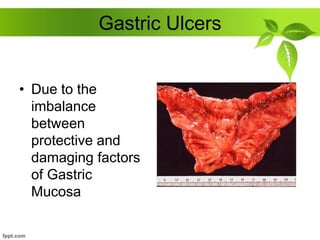
- 5. Gastric Ulcers • Due to the imbalance between protective and damaging factors of Gastric Mucosa
- 6. Stomach Defense Systems • Mucous layer – Coats and lines the stomach – First line of defense • Bicarbonate – Neutralizes acid • Prostaglandins – Hormone-like substances that keep blood vessels dilated for good blood flow – Thought to stimulate mucus and bicarbonate production
- 7. CAUSES of GASTRIC ULCER Atropic Gastritis Duodenogastric bile reflux Gastric Stasis Smoking NSAIDS Steroids HELICOBACTER PYLORI (70%) Lower Socioeconomic group
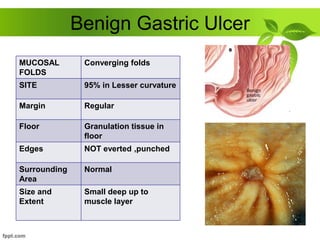
- 8. Benign Gastric Ulcer MUCOSAL FOLDS Converging folds SITE 95% in Lesser curvature Margin Regular Floor Granulation tissue in floor Edges NOT everted ,punched Surrounding Area Normal Size and Extent Small deep up to muscle layer
- 9. Malignant Gastric Ulcer MUCOSAL FOLDS Effacing Mucosal folds SITE Greater curvature Margin Irregular margin Floor Necrotic Slough in the floor Edges Everted Edges Surrounding Area Shows nodules, ulcers and irregularities Size and Extent Large and Deep
- 10. Types of Gastric Ulcer Type I in the andrum, near lesser curvature Type II Combined gastric and duodenal ulcer Type III Prepyloric Type IV Ulcer in the proximal stomach and Cardia 55% 25% 15% 5%
- 11. Gastric Ulcers • Pain occurs 1-2 hours after meals • Pain usually does not wake patient • Accentuated by ingestion of food • Risk for malignancy • Deep and penetrating and usually occur on the lesser curvature of the stomach
- 12. Gastric ulcer >3cm is called GIANT GASTRIC ULCER Gastric Ulcers is equal in both sexes affect older population less common than duodenal ulcers
- 13. Duodenal Ulcers Aetiology HELICOBACTER PYLORI (90%) NSAIDS, Steroids Zollinger Ellison Syndrome Alcohol, Smoking Blood Group O MEN 1 Chronic Pancreatitis
- 14. Duodenal Ulcers • Pain occurs 2-4 hours after meals • Pain wakes up patient • Pain relieved by food • Very little risk for malignancy
- 15. • Most Common in first part of duodenum • Chronic Ulcer penetrates the mucosa and into the muscle coat, leading to fibrosis • Fibrosis ------- Pyloric Stenosis
- 16. ANTERIOR ULCER ---- PERFORATE POSTERIOR ULCER ---- BLEEDS
- 17. GASTRIC ULCER erode LEFT GASTRIC VESSELS and SPLENIC VESSELS DUODENAL ULCER erodes GASTRODUODENAL artery
- 18. • Microscopically, Duodenal Ulcer shows, Destruction of Muscular Coat Base of ulcer with Granulation Tissue Arteries in the region shows ENDARTERITIS OBLITERANS
- 19. General Peptic Ulcer Symptoms PAIN Epigastric ---- Radiating to Back Periodicity Due to spontaneous Healing of ulcer Vomiting Present when stenosis occurs Weight Alteration Gastric loss Duodenal - > Gain Bleeding May present as anemia
- 20. Clinical Features GASTRIC ULCER DUODENAL ULCER Pain after food Intake Pain before food intake Periodicity less Common Periodicity more Common Weight loss +++ Weight Gain+++ Male = Female Male > Female Hemetemesis more Malena more
- 21. INVESTIGATIONS • Esophagogastrodeodenoscopy (EGD) • Upper gastrointestinal series (UGI) (Barium swallow) • Urea Breath Testing • USG
- 22. GASTRODUODENOSCOPY – Endoscopic procedure – Visualizes ulcer crater – Ability to take tissue biopsy to R/O cancer and diagnose H. pylori
- 23. It is fundamental that any gastric ulcer should be regarded as being Malignant, no matter how classically it resemble a benign gastric ulcer Multiple biopsies should be taken, as many as 10 well targeted biopsies
- 24. Biopsy can be taken to look for the presence of Helicobacter Pylori
- 25. Rapid Urease Test C13 or C14 breath test – Client drinks a carbon-enriched urea solution – Excreted carbon dioxide is then measured Faecal Antigen Test
- 26. BARIUM MEAL X Ray of Benign Gastric Ulcer • Outpouching of ulcer crater beyond the gastric contour (exoluminal)
- 27. HAMPTOMs LINE • Overhanging mucosa at the margins of a benign gastric ulcer, project inwards towards the ulcer HAMPTOMs LINE
- 28. • Regular/ Round Margin of the Ulcer Crater STOMACH SPOKE WHEEL PATTERN
- 29. • Converging mucosal folds towards the base of ulcer
- 30. Complications of Peptic Ulcers • Hemorrhage – Blood vessels damaged as ulcer erodes into the muscles of stomach or duodenal wall – Coffee ground vomitus or occult blood in tarry stools • Perforation – An ulcer can erode through the entire wall – Bacteria and partially digested fool spill into peritoneum=peritonitis • Narrowing and obstruction (pyloric) – Swelling and scarring can cause obstruction of food leaving stomach=repeated vomiting
- 31. Medical Management • Provide pain relief – Antacids and mucosa protectors • Eradicate H. pylori infection – Two antibiotics and one acid suppressor • Heal ulcer – Eradicate infection – Protect until ulcer heals • Prevent recurrence – Decrease high acid stimulating foods in susceptible people – Avoid use of potential ulcer causing drugs – Stop smoking AIM
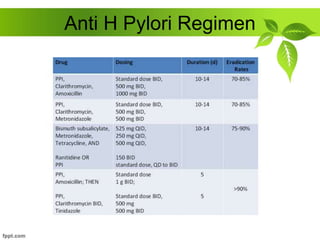
- 32. Anti H Pylori Regimen
- 33. Hyposecretory Drugs • Proton Pump Inhibitors – Suppress acid production • H2-Receptor Antagonists – Block histamine-stimulated gastric secretions • Antacids – Neutralizes acid and prevents formation of pepsin – Give 2 hours after meals and at bedtime • Prostaglandin Analogs – Reduce gastric acid and enhances mucosal resistance to injury • Mucosal barrier fortifiers – Forms a protective coat • Sucralfate
- 34. Surgery • Greatly decreased from 1960 secondary to the discovery of H. pylori • Indication for Surgery – PERFORATION – OBSTRUCTION – HEMORRHAGE – NOT RESPONDING TO MEDICAL TREATMENT
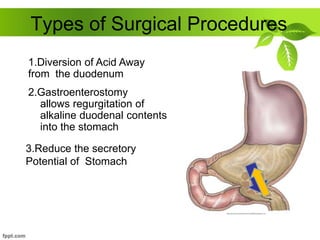
- 35. Types of Surgical Procedures 2.Gastroenterostomy allows regurgitation of alkaline duodenal contents into the stomach 1.Diversion of Acid Away from the duodenum 3.Reduce the secretory Potential of Stomach
- 36. Vagotomy Truncal Vagotomy – Section of the vagus nerve – Reduces the maximal acid output by app 50% Selective Vagotomy Highly Selective Vagotomy Fibres supplying the parietal cells are ligated Nerve of Latarjet which supplies andrum is retained So no drainage proceedure is required in HSV preserved Gastric branches are severed Hepatic branches are preserved
- 37. Drainage Procedures • Pyloroplasty It is a drainage procedure Longitudnal Sectioning of Pyloric Ring Incision is closed transversely
- 38. Gastrojejunostomy Alternative Drainage Procedure to Pyloroplasty Opening the lesser sac and performing anastomosis between the most dependent part of andrum and first jejunal loop.
- 39. Types of Surgical Procedures • Antrectomy – Lower half of stomach (antrum) makes most of the acid – Removing this portion (antrectomy) decreases acid production • Subtotal gastrectomy – Removes ½ to 2/3 of stomach • Remainder must be reattached to the rest of the bowel – Billroth I – Billroth II
- 40. Billroth I Gastrectomy Distal portion of the stomach is mobilised and resected The cut edge of the remnant is partially closed from Lesser Curvature aspect Stoma at greater curvature aspect Gastroduodenal anastomosis done
- 41. Billroth II Gastrectomy The lower portion of the stomach is removed and the remainder is anastomosed to the jejunum Duodenum is closed off by suture of staples High Operative Mortality and Morbidity
- 42. Sequelae of Peptic Ulcer Surgery • Recurrent Ulceration • Small Stomach Syndrome • Bile Vomiting • Early and Late Dumping • Post Vagotomy Diarrhoea • Malignant Transformation • Nutritional Consequences • Gall Stones
- 43. Dumping Syndrome EARLY DUMPING • Rapid emptying of hyperosmolar food and fluids from the stomach into the jejunum • Symptoms – Weakness – Faintness – Palpatations – Fullness – Discomfort – Nausea – diarrhea Rx Dietary manipulation Octreotide before meals Avoid High Carbohydrate Content
- 44. LATE DUMPING It is reactive hypoglycemia CHO load in small bowel ===> rise in blood glucose ===> Insulin levels to rise ===> Secondary Hypoglycemia
- 45. thankyou