Viral host interactions

This document discusses viral-host interactions at the cellular, individual, and community levels. At the cellular level, viruses can cause cell death, malignant transformation, cellular proliferation, or no effect. They also change the cellular architecture by producing inclusion bodies, syncytium formation from cell membrane fusion, and altering host chromosomes. Pathogenesis depends on factors like route of entry, incubation period, host immune response including antibodies and cell-mediated immunity, and non-immunological responses like interferons and temperature. Laboratory diagnosis involves microscopy, antigen demonstration, virus isolation, and serological tests. Immunoprophylaxis uses live attenuated or killed vaccines. Chemoprophylaxis targets specific viral enzymes through nucleoside analogues, protease inhibitors, and
































Viral host interactions
- 1. VIROLOGY PART iii VIRAL – HOST INTERACTIONS Dr.Riyaz Sheriff
- 2. Viral – host interactions • Cellular level • Individual level • Community level @ Cellular level • Cellular changes seen in tissue culture plate may not be seen in clinical infection Cell death Malignant transformation Cellular proliferation No effect
- 3. • Non structural proteins shut down the host protein & DNA synthesis • Large amount of Viral components change the cellular architecture of host cell • Toxic effects • Change in permeability of Host cell AUTOLYSIS • Formation of syncytium d/t fusion of adjacent cell membranes • Viral antigens will confer newer properties on host cell (cell adsorption, oncogenesis) • Changes in the host chromosome ( Measles, Mumps, Adenovirus, CMV & Varicella) • Inclusion bodies
- 4. Inclusion bodies • Structures with distinct size, shape , location and staining properties • Can be seen under light microscope after staining • May be seen in cytoplasm or nucleus • Generally acidophilic in nature – Pink in colour on staining with Giemsa or Eosin methylene blue stains • Some may be basophilic as well
- 5. Inclusion bodies • Helps in diagnosis – Negri bodies – intra cytoplasmic inclusion – Rabies – Guarnieri bodies – vaccinia – Bollinger bodies – fowl pox – Molluscum bodies – molluscum contagiosum – Cowdry type A – Herpes virus , Yellow fever virus – Cowdry type B – Adeno virus, Polio virus • Inclusion bodies my be an aggregate of virions or collection of viral antigens or the degenerative changes produced by viral infection.
- 6. Negri bodies – Rabies – Intracytoplasmic
- 7. Guarnieri bodies – vaccinia
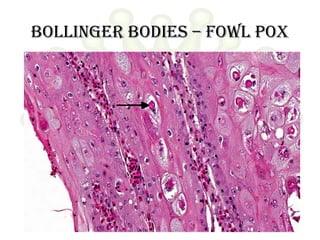
- 8. Bollinger bodies – fowl pox
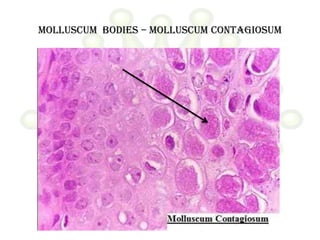
- 9. Molluscum bodies – molluscum contagiosum
- 10. Cowdry type A Hepatocyte with a large intranuclear inclusion body. Surrounded by a clear halo
- 11. Cowdry type b
- 12. Pathogenesis of viral infection • Inapparent • Apparent – Acute – Subacute – Chronic • Latent • Persistent tolerant infections : Congenital / Neonatal infections • Oncogenic virus • HIV
- 13. Route of entry • Respiratory tract (Most common) – Multiply locally Blood/Lymph Extensive multiplication Disease. – Small pox, chicken pox – Influenza , Rhinovirus (stay in respiratory tract itself) • Alimentary tract – All enveloped viruses are destroyed by bile – Rhinovirus is inactivated by gastric juice – Enterovirus, adenovirus, reo virus, hepatitis virus – Some multiply in GIT and transported to target organs (eg.Polio virus) • Genital tract • Conjunctiva • Skin • Vertical transmission – Mother to baby
- 14. Route of entry • Skin – Produce few local lesions – Papilloma, vaccinia, cowpox & molluscum contagiosum. – Viruses can enter through break in skin – Abrasions – Papiloma virus – Insect bites – Arbovirus – Animal bites – Rabies – Injections – Hepatitis • Genital tract – Human immuno deficiency virus
- 15. Route of entry • Conjunctiva – Local disease – Adenovirus – Systemic disease – Measles • Vertical transmission – Mother to baby – May occur at any stage till birth – Usally leads to fetal death and abortion – Maldevelopment – Rubella and Cytomegalovirus – Many tumor virus spread via this route
- 16. Spread of virus in the body • Studied by Fenner using mouse pox as a model
- 17. Mouse pox virus Enters through skin Local Multiplication Skin & Lymphatics Lymph Nodes Blood (Primary Viremia) Spleen , Liver (Central foci ) Extensive multiplication Spills into blood(Secondary Viremia) Clinical symptoms Virus reaches target organ Multiplication CLINICAL DISEASE
- 18. Incubation period • Time taken for virus to spread from site of entry to the organs of viral multiplication and causation of disease. • Localized diseases : Shorter incubation period • Systemic diseases : Longer incubation period • Incubation period shorter when directly introduced into blood stream
- 19. Host response Depends on 1. Virulence of the infecting strain 2. Resistance of the host » Immunological • Humoral • Cell mediated immunity » Non specific • Interferon production • Body temperature • Age • Malnutrition
- 20. • Viral infection liberates – Surface antigens – Internal antigens – Non structural antigens • Early proteins – Humoral immunity • IgG • IgM • IgA Mucosal surface Blood and Tissue
- 21. Immunoglobulins on viruses • Prevents attachment of virus to cell • Enhances viral degradation • Prevents release of virions from infected cell Immunoglobulin + Complement Surface damage of enveloped virions Cytolysis of virus infected cells
- 22. Role of antibodies • Role of antibodies in viral infection is limited • Antibody to internal antigen Non neutralizing • Antibody to surface antigen varying neutralization • Some antibodies can paradoxically increase infectivity • May contribute to Pathogenicity • Antibody may result in – Complement dependent cell injury – Immune complex type tissue injury
- 23. Role of cmi • Plays a major role in viral infection • Helps in recovery from viral infection • Can cause tissue damage as well • Deficient CMI increase in Herpes, Pox, Measles • Most often an infection provides long lasting immunity
- 24. Non immunological responses Macrophages phagocytose virus in blood. Body temperature : > 39°C inhibits most virus Exception – Herpes simplex – fever blisters Hormones : Corticosteroids enhance viral infection. Due to depression of immune system & inhibition of interferon synthesis Malnutrition Age
- 25. Interferons • Family of host coded proteins • No direct action on virus • Acts on host cells to make them refractory o viral infection. • On exposure to interferon cells produce TIP (Translation Inhibition Protein) inhibits translation of viral mRNA • Does not affect translation of host mRNA • Interferons are species specific. • RNA viruses are better inducers of interferon production • Temperature of > 40°C induces interferon secretion • Steroids and increased O2 tension decrease interferon synthesis • Synthesis starts in about 30mins of induction and reaches peak by 6-12 hours.
- 26. Interferons • α leucocytes • ß fibroblasts • Ɣ T-Lymphocytes • Inactivated by proteolytic enzymes • Resist 56°C – 60°C for 30-60mins • α & ß are resistant at pH range of 2-10 • Ɣ is labile at pH of 2 • Non toxic • Poorly antigenic • Cannot be estimated by routine serological methods
- 27. Use of Interferons • Ideal candidate for prophylaxis and treatment – Non toxic – Non antigenic – Diffuses freely in the body – Wide spectrum of antiviral activity • Drawback species specific • Current use URTI, Warts, Herpetic keratitis & anticancer agent in lymphomas
- 28. Biological effects of interferons • Anti-Viral : resistance to infection • Anti –Microbial: Resistance to intracellular infections (Toxoplasma, Chlamydia, Malaria) • Cellular effects : Inhibition of cell growth and proliferation, Increased expression of MHC antigens on cell surface • Immunoregulatory : – Increases activity of Natural killer (NK) calls and T cells. – Activates cell destruction activity of macrophage – Moderates antibody formation – Activates suppressor T cells – Suppresses DTH
- 29. Lab diagnosis • Microscopy : Demonstration of virus by electron microscopy Demonstration of inclusion bodies Fluorescent antibody techniques • Demonstration of viral antigen: Possible when viral antigens are abundant in the lesion Precipitation in gel Immunofluorescence CIE RIA ELISA PCR
- 30. Lab diagnosis • Isolation of virus : • Need proper transport media at appropriate temperature • Processing to remove bacterial contaminants • Inoculation in eggs • Animal inoculation • Tissue culture • Virus isolation has to be correlated with clinical history Identified by Neutralization tests
- 31. Lab diagnosis • Serological diagnosis : • Rise in titre of antibodies during course of disease • Examine paired sera – Acute – Convalescent (10-14 days later ) • When IgM alone is tested Single sample is enough – Neutralization test – Complement fixation – ELISA – Hemagglutination Inhibition
- 32. Immunoprophylaxis • Infection / vaccine Prolonged and effective immunity • Live vaccines more effective than killed vaccines • Successful Live vaccines – Small pox vaccine – Yellow fever vaccine – Polio Vaccine ( Sabin) • Killed vaccines prepared by inactivating viruses using Heat, Phenol, Formalin or BPL • Subunit vaccines – Hepatitis B
- 33. Live attenuated vaccines Advantages • Single dose • Administered by route of natural infection • Induce immunoglobulins • Induce CMI • Long lasting immunity • Economical • Apt for mass immunizations Disadvantages • Remote chance of reactivation of virus • Cannot be used in immunocompramised • Existence of other viruses may result in lessened immune response • Needs proper cold chain Killed vaccines • Safe • Stable • Can be given as combined vaccines • Multiple doses • Does not induce local immunity or cell mediated immunity
- 34. Chemoprophylaxis • Challenge Viruses are strictly intracellular , use host mechanisms for replication. Hence therapy would destroy host cell as well • Answer Selective inhibition of viral enzymes – Attachment – Transcription of viral nucleic acid – Translation – Replication – Viral assembly – Release
- 35. Antiviral agents • 1960 : First antiviral – Pox virus : Small pox eradicated by vaccination • 1962 : Idoxyuridine : Herpes Keratitis • 1970 : Acyclovir : effective in Herpes • Nucleoside analogues – Deoxyuridines • Idoxyuridine Herpetic keraitis • Trifluridine Less toxic • Bromovinyldeoxyuridine Herpes & Varicella – Adenine arabinoside • Herpetic keratitis • Herpes simplex • VZV – Acyclovir herpes – Ganciclovir Cytomegalovirus – Zidovudine HIV : inhibits viral reverse transcriptase
- 36. • Protease inhibitors – Saquinavir – Ritonovir – Indinavir • Others – Amantidine – blocks cell penetration by influenza A but not by B&C Antiviral agents