
















































growth and development of mandible
- 1. Dr SHILPA JOY V S Dental College 13/1/2017 99
- 2. CONTENTS Introduction Anatomy of mandible Evolution of mandible Mandibular growth mechanisms-Brief history Prenatal growth of mandible Postnatal development Growth progression-mechanism & site Age changes in mandible Theories of mandibular growth Problems of mandibular growth and orthodontic significance Conclusion References 23/1/2017 99
- 3. INTRODUCTION The human mandible has no one design for life.Rather it adapts and remodels through the seven stages of life,from the slim arbiter of things to come in the infant,through a powerful dentate machine and even weapon in the full flesh of maturity ,to the pencil thin,porcelain like problem that we struggle to repair in the adversity of old age –D.E POSWILLO It is attached only by ligaments and muscles to immovable bones of the skull. The temporomandibular or ginglymo-diarthroidal joints are the only visible movable articulations in the head. The rest of the bones of the skull move in union when the head is moved as a whole. 33/1/2017 99
- 4. DEFINITIONS RELATED TO GROWTH Moss: change in morphological parameters which is measurable. Moyers: Quantitative aspect of biological development per unit of time. Todd: An increase in size. Krogman: increase in size change in proportions and progressive complexity J.S. Huxley: The self multiplications of living substance Meridith:entire series of sequential anatomic and Physiologic changes taking place from beginning of pre natal life to serenity DEVELOPMENT Todd:progress towards maturity Moyers:All naturally occuring unidirectional changes in the life of an individual from its existence as a single cell to its elaboration as a multifunctional unit terminating in death 43/1/2017 99
- 6. 63/1/2017 99
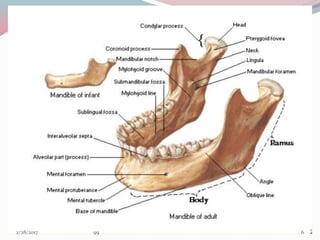
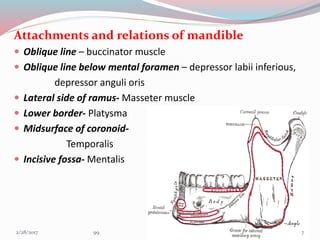
- 7. Attachments and relations of mandible Oblique line – buccinator muscle Oblique line below mental foramen – depressor labii inferious, depressor anguli oris Lateral side of ramus- Masseter muscle Lower border- Platysma Midsurface of coronoid- Temporalis Incisive fossa- Mentalis 73/1/2017 99
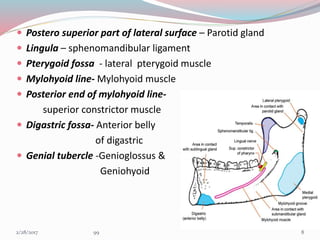
- 8. Postero superior part of lateral surface – Parotid gland Lingula – sphenomandibular ligament Pterygoid fossa - lateral pterygoid muscle Mylohyoid line- Mylohyoid muscle Posterior end of mylohyoid line- superior constrictor muscle Digastric fossa- Anterior belly of digastric Genial tubercle -Genioglossus & Geniohyoid 83/1/2017 99
- 9. EVOLUTION OF MANDIBLE The agnatha, the earliest type of vertebrate, had its mouth opening on the ventral side anteriorly along the vertebral axis. They did not have jaws The Placoderms, had 7 arches.The first arch was lost.Their new first arch became the Mandibular arch that formed the jaws.The upper half of mand.arch became palatoquadrate cartilage and lower half became the mandibular or meckels cartilage In Elasmobrancs,the jaws were formed by mandibular arch (arch 1) & hyoid arch(arch 2) The upper half of hyoid arch became hyomandibular ligament and lower half became hyoid cartilage 93/1/2017 99
- 10. In amphibians the hyomandibular ligament became the stapes .They had a dentary bone in the anterior end of the original cartilaginous jaw. At its posterior extremity it articulated with the quadrate bone In reptiles like early synapsid ,that gave rise to mammals ,the jaw joint is formed by the articular(lower) & quadrate(upper) bones.The joint was a simple hinge at the posterior of jaw In mid and late synapsid reptiles,the dentary bone (lower jaw) increase in size as muscle and bite force increased,but force on the joint decreased as the muscle insertion point shifted to allow greater jaw mobility The articular and quadrate bones at the jaw joint became smaller and was loosely attached with the dentary 103/1/2017 99
- 11. The coronoid process of dentary bone formed to accommodate these changing forces Ultimately in mammals,the jaw joint shifted from a articular-quadrate joint to a dentary-squamosal joint.the condylar process formed to create a new articulating surface 113/1/2017 99
- 12. MANDIBULAR GROWTH PATTERNS- A HISTORY • HUNTER (1771) compared a series of dried mandibles and concluded that in order to attain space for permanent molar teeth the mandible must grow by posterior apposition of ramus accompanied by anterior ramus resorption. • HUMPHRY (1866) studied growth of mandible by inserting metal rings in the anterior and posterior margins of mandibular ramus in growing pig.Rings placed on posterior border became more deeply embedded but rings placed on anterior surface were released • BRASH (1924) fed pigs the madder plant root(alizarin ) which labeled appositional growth WEINMAN AND SICHER (1940) with the help of longitudinal cephalometrics and evidence from experiments of animals, focused attention on the mandibular condyle as a major factor in growth of the mandible. A STUDY OF POSTNATAL GROWTH OF HUMAN MANDIBLE-DONALD H ENLOW,DAVID B HARRIS AJODO,JAN 1964 123/1/2017 99
- 13. BRODIE believed that superior and posterior growth of the condyle along with apposition of the posterior border of the ramus and alveolar border resulted in development of mandible. RICKETTS(1950)by superimpositions on lower border of the mandible showed that the condyle followed a superior and posterior course. He also noted that the mandibular growth was not same and that the relationship of the mandibular plane to the Frankfort Horizontal plane was changing about one degrees every 3 yrs in a typical facial pattern. MOSS(1960) envisioned the growth of the mandible as a logarithmic spiral constructed via the path of the mandibular nerve. 133/1/2017 99
- 14. BJORK (1963 )conducted a study with tantalum implants and suggested that 1. Growth in length of the mandible occurs at the condyles. 2. The anterior aspect of chin is extremely stable 3. The thickening of the symphysis takes place by appostion on its posterior surface and lower border which contributes to increase in height of symphysis. 4. At the region of the condyles there is upward and forward curving growth. 5. The mandibular canal is not remodeled and the trabaculae related to the canal are stationary. Hence the curvature of the mandibular canal generally reflects the earlier shape of the mandible VARIATION IN GROWTH PATTERN OF HUMAN MANDIBLE;A LONGITUDINAL RADIOGRAPHIC STUDY BY IMPLANT METHOD-ARNE BJORK ;J DENT RES 1963 . 143/1/2017 99
- 15. Growth & development of an individual can be divided in to Pre-natal Post-natal Period of Ovum 1-14th day Period of embryo 14th – 56th day Period of Fetus 56th – 270th day 153/1/2017 99
- 16. PRENATAL GROWTH PERIOD OF OVUM Fertilization-Ampulla of uterine tube zygote mitosis Cluster of cells(Blastomere) mitosis Morula(16 cell structure) Blastocyst 163/1/2017 99
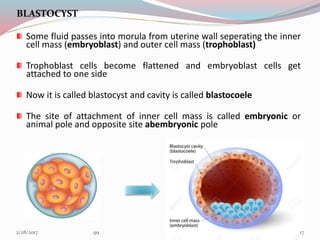
- 17. BLASTOCYST Some fluid passes into morula from uterine wall seperating the inner cell mass (embryoblast) and outer cell mass (trophoblast) Trophoblast cells become flattened and embryoblast cells get attached to one side Now it is called blastocyst and cavity is called blastocoele The site of attachment of inner cell mass is called embryonic or animal pole and opposite site abembryonic pole MORULA 173/1/2017 99
- 18. PERIOD OF EMBRYO PRESOMITE PERIOD(8-20th day) Trophoblastic layer differentiate into synctiotrophoblast and cytotrophoblast layers SYNCTIOTROPHOBLAST- Outer cells that invades endometrium and its vessels to establish maternal blood circulation to developing embryo-UTEROPLACENTAL CIRCULATION PRESOMITE SOMITE POSTSOMITE 183/1/2017 99
- 19. INNER CELL MASS Differentiation BILAMINAR DISC BLASTOCYSTIC CAVITY is now called as primitive yolk sac AMNIOTIC CAVITY develops between epiblast and cytotrophoblast HYPOBLAST Squamous /cuboidal EPIBLAST Columnar cells 193/1/2017 99
- 20. Extra embryonic mesoderm(EEM) formed of loose connective tissue , differentiate between developing embryo and cytotrophoblast Chorionic cavity is formed by fusion of number of lacunae that develop in EEM Expansion of chorionic cavity reduces size of primitive yolk sac,forming secondary yolk sac, occurs by end of second week 3rd week- Gastrulation occurs Bilaminar disc-Trilaminar disc 203/1/2017 99
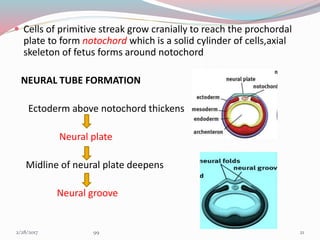
- 21. Cells of primitive streak grow cranially to reach the prochordal plate to form notochord which is a solid cylinder of cells,axial skeleton of fetus forms around notochord NEURAL TUBE FORMATION Ectoderm above notochord thickens Neural plate Midline of neural plate deepens Neural groove 213/1/2017 99
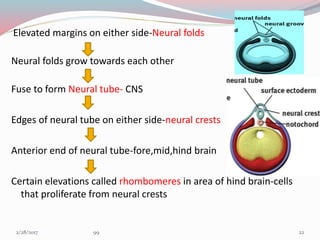
- 22. Elevated margins on either side-Neural folds Neural folds grow towards each other Fuse to form Neural tube- CNS Edges of neural tube on either side-neural crests Anterior end of neural tube-fore,mid,hind brain Certain elevations called rhombomeres in area of hind brain-cells that proliferate from neural crests 223/1/2017 99
- 23. NEURAL CREST CELLS Forms from neuro ectoderm Migrate & differentiate extensively with in the developing embryo Spinal & cranial sensory ganglia, Sympathetic neurons, Schwann cells, pigment cells & meninges Most of the connective tissue of the head is formed Migration is essential for development of teeth & face All the tissues of teeth (except enamel) & its supporting apparatus are derived directly from these cells 233/1/2017 99
- 24. SOMITE PERIOD(21ST -31ST day of IUL) Rapid growth of cranial end of embryo,caudal end lags behind- CEPHALOCAUDAL GRADIENT OF GROWTH Head-1/2 of total embryonic disk length BRANCHIAL /PHARYNGEAL ARCHES In specific areas,the migrating and rapidly proliferating ectomesenchyme cells develops elevation between ectoderm and endoderm 4th week of IUL Elevations seen in ventral foregut 5th arch perishes Formation of 6 pharyngeal arches (bilaterally) Finally 5 arches remain 243/1/2017 99
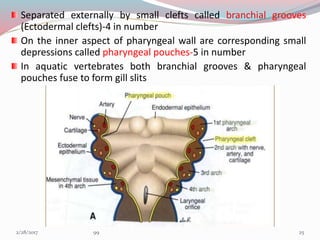
- 25. Separated externally by small clefts called branchial grooves (Ectodermal clefts)-4 in number On the inner aspect of pharyngeal wall are corresponding small depressions called pharyngeal pouches-5 in number In aquatic vertebrates both branchial grooves & pharyngeal pouches fuse to form gill slits 253/1/2017 99
- 26. 263/1/2017 99
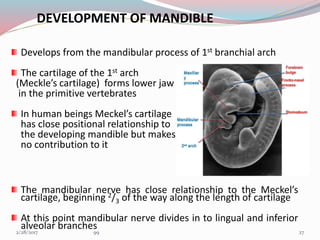
- 27. DEVELOPMENT OF MANDIBLE Develops from the mandibular process of 1st branchial arch The cartilage of the 1st arch (Meckle’s cartilage) forms lower jaw in the primitive vertebrates In human beings Meckel’s cartilage has close positional relationship to the developing mandible but makes no contribution to it The mandibular nerve has close relationship to the Meckel’s cartilage, beginning 2/3 of the way along the length of cartilage At this point mandibular nerve divides in to lingual and inferior alveolar branches 273/1/2017 99
- 28. At around 36-38 days of IUL there is ectomesenchymal condensation Some mesenchymal cells enlarges,acquire a basophilic cytoplasm and form osteoblasts Osteoblast secrete a gelatinous matrix called osteoid and results in ossification of osteogenic membrane The resulting intramembranous bone lies lateral to meckels cartilage of mandibular arch 283/1/2017 99
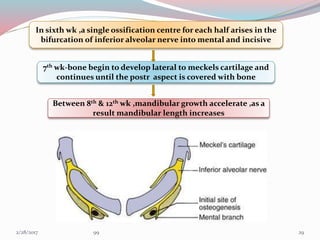
- 29. In sixth wk ,a single ossification centre for each half arises in the bifurcation of inferior alveolar nerve into mental and incisive 7th wk-bone begin to develop lateral to meckels cartilage and continues until the postr aspect is covered with bone Between 8th & 12th wk ,mandibular growth accelerate ,as a result mandibular length increases 293/1/2017 99
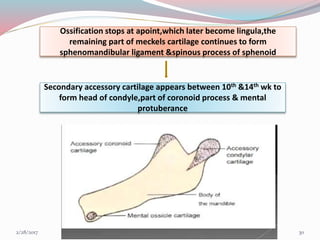
- 30. Ossification stops at apoint,which later become lingula,the remaining part of meckels cartilage continues to form sphenomandibular ligament &spinous process of sphenoid Secondary accessory cartilage appears between 10th &14th wk to form head of condyle,part of coronoid process & mental protuberance 303/1/2017 99
- 31. FATE OF MECKELS CARTILAGE Posterior extremity forms malleus, incus & sphenomandibular ligament Most of the cartilage is absorbed except for some portion in midline which may cause endochondral ossification FETAL PERIOD Endochondral bone formation seen only in 3 areas • Condylar process • Coronoid process • Mental region 313/1/2017 99
- 32. Condylar process About 5th week of I.U.L. area of mesenchymal condensation above the ventral part of developing mandible About 10th wk develops into cone shaped cartilage By 14th week starts ossification By 4 months migrates inferiorly and fuses with ramus 4th month onwards replaced by bone but proximal end persists into adulthood acting as Growth cartilage & Articular cartilage Condylar head separated from temporal bone by thin disc of connective tissue – future articular disc 323/1/2017 99
- 33. Coronoid process By 10th to 14th week of I.U.L. secondary cartilages seen in region of coronoid This cartilage becomes incorporated into expanding intramembranous bone of ramus and disappears before birth Mental region Secondary cartilages seen on both sides -- ossify by 7th wk I.U.L. They ossify to form mental ossicles in fibrous tissue of symphysis and later on gets incorporated into it. 333/1/2017 99
- 34. POST NATAL DEVELOPMENT MANDIBLE AT BIRTH MANDIBULAR GROWTH-FIRST YEAR GROWTH PROGRESSION AFTER FIRST YEAR- MECHANISM & SITE 343/1/2017 99
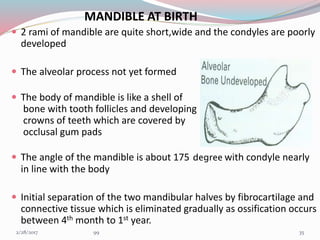
- 35. MANDIBLE AT BIRTH 2 rami of mandible are quite short,wide and the condyles are poorly developed The alveolar process not yet formed The body of mandible is like a shell of bone with tooth follicles and developing crowns of teeth which are covered by occlusal gum pads The angle of the mandible is about 175 degree with condyle nearly in line with the body Initial separation of the two mandibular halves by fibrocartilage and connective tissue which is eliminated gradually as ossification occurs between 4th month to 1st year. 353/1/2017 99
- 36. MANDIBULAR GROWTH DURING FIRST YEAR Appositional growth especially active at Alveolar border Distal and superior surface of ramus Condyle Lower border of mandible Lateral surface of mandible After first year growth becomes more selective,condyle shows considerable activities , mandible moves and grows forward and downward 363/1/2017 99
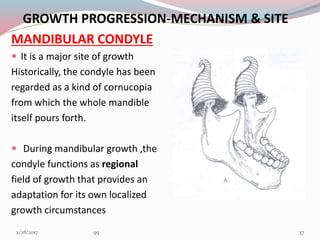
- 37. GROWTH PROGRESSION-MECHANISM & SITE MANDIBULAR CONDYLE It is a major site of growth Historically, the condyle has been regarded as a kind of cornucopia from which the whole mandible itself pours forth. During mandibular growth ,the condyle functions as regional field of growth that provides an adaptation for its own localized growth circumstances 373/1/2017 99
- 38. The condylar cartilage is a secondary type of cartilage Its real contribution is to provide regional adaptive growth Main functional role of condyle is (1) provides a pressure tolerant articular contact (2) it makes possible a multidimensional growth capacity in response to ever-changing, developmental conditions and variations. The condylar growth mechanism itself is a clear-cut process. Cartilage is a special non-vascular tissue and is involved because variable levels of compression occur at its articular contact with temporal bone 383/1/2017 99
- 39. An endochondral growth mechanism is required ,because the condyle grow in a direction towards its articulation in the face of direct pressure Intramembranous type couldn’t operate because the periosteal mode of osteogenesis is not pressure adapted In Figure the endochondral bone tissue (b) , formed in association with the condylar cartilage (a) is laid down only in medullary portion The enclosing bony cortices (c) are produced by periosteal- endosteal osteogenic activity 393/1/2017 99
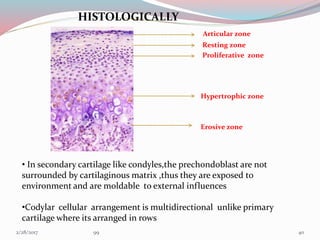
- 40. HISTOLOGICALLY Articular zone Resting zone Proliferative zone Hypertrophic zone Erosive zone • In secondary cartilage like condyles,the prechondoblast are not surrounded by cartilaginous matrix ,thus they are exposed to environment and are moldable to external influences •Codylar cellular arrangement is multidirectional unlike primary cartilage where its arranged in rows 403/1/2017 99
- 41. Anterior margin of condylar neck is depository, this surface is part of sigmoid notch Posterior edge which grades into posterior border of ramus is also depository The lingual and buccal sides of neck characteristically have a resorptive surface. This is because condyle is quite broad and neck is narrow 413/1/2017 99
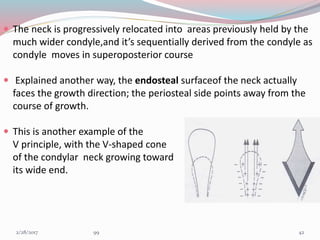
- 42. The neck is progressively relocated into areas previously held by the much wider condyle,and it’s sequentially derived from the condyle as condyle moves in superoposterior course Explained another way, the endosteal surfaceof the neck actually faces the growth direction; the periosteal side points away from the course of growth. This is another example of the V principle, with the V-shaped cone of the condylar neck growing toward its wide end. 423/1/2017 99
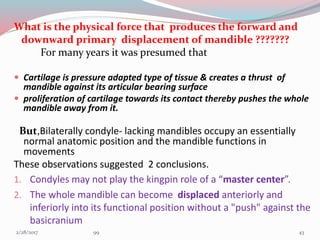
- 43. What is the physical force that produces the forward and downward primary displacement of mandible ??????? For many years it was presumed that Cartilage is pressure adapted type of tissue & creates a thrust of mandible against its articular bearing surface proliferation of cartilage towards its contact thereby pushes the whole mandible away from it. But,Bilaterally condyle- lacking mandibles occupy an essentially normal anatomic position and the mandible functions in movements These observations suggested 2 conclusions. 1. Condyles may not play the kingpin role of a “master center”. 2. The whole mandible can become displaced anteriorly and inferiorly into its functional position without a "push" against the basicranium 433/1/2017 99
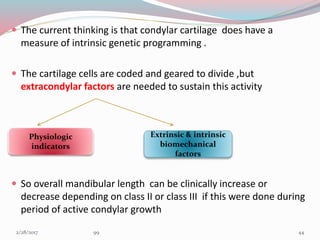
- 44. The current thinking is that condylar cartilage does have a measure of intrinsic genetic programming . The cartilage cells are coded and geared to divide ,but extracondylar factors are needed to sustain this activity So overall mandibular length can be clinically increase or decrease depending on class II or class III if this were done during period of active condylar growth Physiologic indicators Extrinsic & intrinsic biomechanical factors 443/1/2017 99
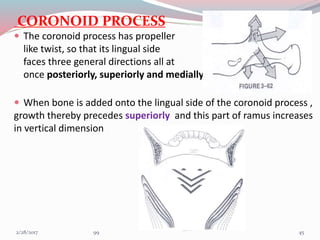
- 45. CORONOID PROCESS The coronoid process has propeller like twist, so that its lingual side faces three general directions all at once posteriorly, superiorly and medially. When bone is added onto the lingual side of the coronoid process , growth thereby precedes superiorly and this part of ramus increases in vertical dimension 453/1/2017 99
- 46. These same deposits of bone on the lingual side also bring about a posterior direction of growth movement . Produces backward movement of two coronoid process even though deposits on the inside (lingual) surface. These same deposits on the lingual side also bring about medial direction of growth in order to lengthen corpus Area occupied by anterior part of ramus in mandible 1 becomes relocated and remodeled into posterior part of corpus in mandible 2. 463/1/2017 99
- 47. CORPUS / BODY OF MANDIBLE Outer surface-depository & medial surface(inferior aspect)- Resorptive,remodelling is in the form of ‘L’ Depository area -from the superior half of medial surface of corpus to anterior half of medial surface of ramus(below coronoid) Resorptive area –from inferior half of medial surface of corpus to posterior half of medial surface of ramus (below condyle) 473/1/2017 99
- 48. RAMUS At birth the two rami of mandible are quite short, they grow by the process of direct surface apposition and remodeling. THE PRINCIPLE GROWTH VECTORS ARE IN POSTERIOR & SUPERIOR DIRECTION Resorption occurs on the anterior surface of ramus while bone deposition occurs on posterior surface. Bone growth occurs at the mandibular condyle and along the posterior part of ramus to the same extent as anterior part has undergone resorption 483/1/2017 99
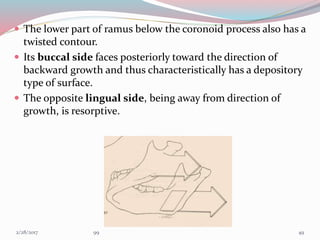
- 49. The lower part of ramus below the coronoid process also has a twisted contour. Its buccal side faces posteriorly toward the direction of backward growth and thus characteristically has a depository type of surface. The opposite lingual side, being away from direction of growth, is resorptive. 493/1/2017 99
- 50. IMPORTANCE OF RAMUS It positions the lower arch in occlusion with the upper. It is continuously adaptive to the multitude of changing craniofacial conditions. Attach the mastication muscle and must accommodate the increasing mass of masticatory muscle inserted into it. Bridges the pharyngeal compartment. The horizontal breadth of ramus determines the anteroposterior positioning of lower arch. Height of ramus accommodates the vertical dimension and growth of nasal and masticatory components of face. Remodeling and relocation give space to accommodate erupting permanent molar. 503/1/2017 99
- 51. RAMUS UPRIGHTING Greater amounts of bone additions on the inferior part of the posterior border than on the superior part. A correspondingly greater amount of matching resorption on the anterior border takes place inferiorly than superiorly. A "remodeling" rotation of ramus alignment thus occurs. In diagram the pharynx enlarges horizontally from a to a’ . The ramus enlarges correspondingly from b to b’ Angle c is reduced to c’ to accommodate the vertical increase,which allows for considerable extent of vertical nasomaxillary growth 513/1/2017 99
- 52. Vertical lengthening of the ramus continues to take place after horizontal ramus growth slows or ceases Resorption takes place on the upper part of the posterior border. A forward growth direction can occur on the anterior border in the upper part of the coronoid process. A posterior direction of remodeling takes place in the lower part of the posterior border,this result in more upright alignment and longer vertical dimension of ramus without increase in breadth In fig mandible a is superimposed over b remodeling changes outlined above serve simply to alter the ramus angle without increasing its breadth 523/1/2017 99
- 53. • The growth and remodeling changes of both ramus and middle cranial fossa produces lowering of mandibular arch .This accommodate vertical expansion of nasomaxillary complex . • A vertical imbalance thus occurs ,this ‘opens’ anterior bite,only the first and second molars are in occlusal contact • The amount of upward mandibular tooth drift is much less than the downward drift and displacement of maxillary teeth. • This is one of the several reason why orthodontic purpose, often attack maxillary dentition ,eventhough given malocclusion can be largely based on improper positioning of mandible 533/1/2017 99
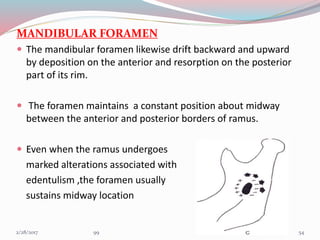
- 54. MANDIBULAR FORAMEN The mandibular foramen likewise drift backward and upward by deposition on the anterior and resorption on the posterior part of its rim. The foramen maintains a constant position about midway between the anterior and posterior borders of ramus. Even when the ramus undergoes marked alterations associated with edentulism ,the foramen usually sustains midway location 543/1/2017 99
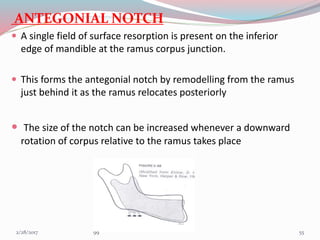
- 55. ANTEGONIAL NOTCH A single field of surface resorption is present on the inferior edge of mandible at the ramus corpus junction. This forms the antegonial notch by remodelling from the ramus just behind it as the ramus relocates posteriorly The size of the notch can be increased whenever a downward rotation of corpus relative to the ramus takes place 553/1/2017 99
- 56. ANTEGONIAL NOTCH –CLINICAL SIGNIFICANCE Deep notched subjects have retrusive mandible with shorter corpus, less ramus height and increase gonial angle. Mandibular growth directions in deep notched patients were more vertically directed as measured by facial axis and the mandibular plane angle. Deep notched subjects had longer total facial height and longer lower facial height,Smaller saddle angle Deep notch patients required a longer duration of orthodontic treatment. 563/1/2017 99
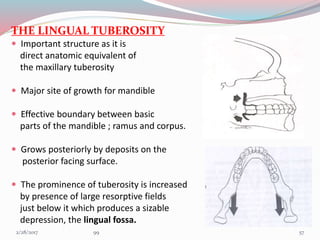
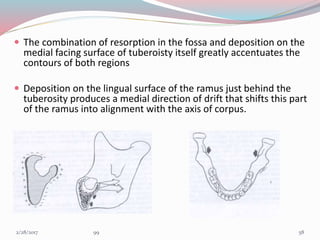
- 57. THE LINGUAL TUBEROSITY Important structure as it is direct anatomic equivalent of the maxillary tuberosity Major site of growth for mandible Effective boundary between basic parts of the mandible ; ramus and corpus. Grows posteriorly by deposits on the posterior facing surface. The prominence of tuberosity is increased by presence of large resorptive fields just below it which produces a sizable depression, the lingual fossa. 573/1/2017 99
- 58. The combination of resorption in the fossa and deposition on the medial facing surface of tuberoisty itself greatly accentuates the contours of both regions Deposition on the lingual surface of the ramus just behind the tuberosity produces a medial direction of drift that shifts this part of the ramus into alignment with the axis of corpus. 583/1/2017 99
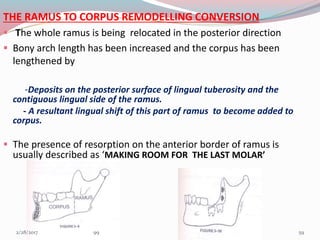
- 59. THE RAMUS TO CORPUS REMODELLING CONVERSION The whole ramus is being relocated in the posterior direction Bony arch length has been increased and the corpus has been lengthened by -Deposits on the posterior surface of lingual tuberosity and the contiguous lingual side of the ramus. - A resultant lingual shift of this part of ramus to become added to corpus. The presence of resorption on the anterior border of ramus is usually described as ‘MAKING ROOM FOR THE LAST MOLAR’ 593/1/2017 99
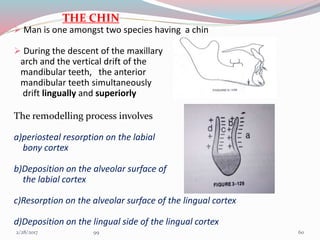
- 60. THE CHIN Man is one amongst two species having a chin During the descent of the maxillary arch and the vertical drift of the mandibular teeth, the anterior mandibular teeth simultaneously drift lingually and superiorly The remodelling process involves a)periosteal resorption on the labial bony cortex b)Deposition on the alveolar surface of the labial cortex c)Resorption on the alveolar surface of the lingual cortex d)Deposition on the lingual side of the lingual cortex 603/1/2017 99
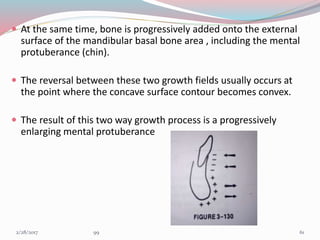
- 61. At the same time, bone is progressively added onto the external surface of the mandibular basal bone area , including the mental protuberance (chin). The reversal between these two growth fields usually occurs at the point where the concave surface contour becomes convex. The result of this two way growth process is a progressively enlarging mental protuberance 613/1/2017 99
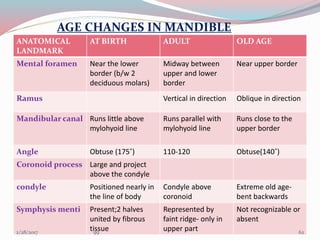
- 62. AGE CHANGES IN MANDIBLE ANATOMICAL LANDMARK AT BIRTH ADULT OLD AGE Mental foramen Near the lower border (b/w 2 deciduous molars) Midway between upper and lower border Near upper border Ramus Vertical in direction Oblique in direction Mandibular canal Runs little above mylohyoid line Runs parallel with mylohyoid line Runs close to the upper border Angle Obtuse (175˚) 110-120 Obtuse(140˚) Coronoid process Large and project above the condyle condyle Positioned nearly in the line of body Condyle above coronoid Extreme old age- bent backwards Symphysis menti Present;2 halves united by fibrous tissue Represented by faint ridge- only in upper part Not recognizable or absent 623/1/2017 99
- 63. THEORIES OF MANDIBULAR GROWTH GENETIC THEORY:- This theory states that all growth is compelled by genetic influence ie: genetic encoding of mandible determines its growth. CARTILAGENOUS THEORY This theory states that the cartilage is the primary determinant of skeletal growth while bone responds secondarily & passively. According to this theory, the condyle by means of endochondral ossification deposits bone, which tends to grow the mandible. 633/1/2017 99
- 64. ENLOW’S EXPANDING ‘V’ PRINCIPLE This theory states that many facial bones or a part of the bone follows a ‘v’ pattern of enlargement. Deposition is in the inner surface of of ‘v’ . Resorption is seen along the outer surface of ‘v’. CORONOID PROCESS: Deposition –lingualsurface, Resorption-buccal CONDYLE PROCESS: Deposition-ant. & post. Margins, Resorption-buccal & lingual surfaces 643/1/2017 99
- 65. ENLOW’S COUNTERPART PRINCIPLE This principle states that growth of any given facial or cranial part relates specifically to other structural & geometric counterpart in the face & cranium 653/1/2017 99
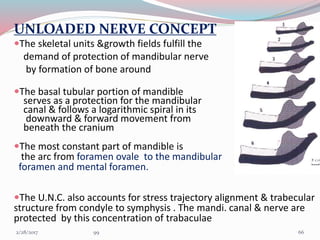
- 66. UNLOADED NERVE CONCEPT The skeletal units &growth fields fulfill the demand of protection of mandibular nerve by formation of bone around The basal tubular portion of mandible serves as a protection for the mandibular canal & follows a logarithmic spiral in its downward & forward movement from beneath the cranium The most constant part of mandible is the arc from foramen ovale to the mandibular foramen and mental foramen. The U.N.C. also accounts for stress trajectory alignment & trabecular structure from condyle to symphysis . The mandi. canal & nerve are protected by this concentration of trabaculae 663/1/2017 99
- 67. SERVO SYSTEM THEORY Control of primary cartilages takes a cybernetic form of ‘command’ whereas control of secondary cartilage like condyle is comprised of both direct effect of cell multiplication and also indirect effects Theories of craniofacial growth in the postgenomic area ;semin ortho 2005 ,11:172-83 MUSCLE FUNCTIONS actuator ANTERIOR GROWTH OF MIDFACE Reference input OCCLUSAL DEVIATION comparator Regulation of inputs-CNS controller TRIGGERS – PROPRIOCEPTIVE RECEPTORS(MUSCLES & PERIODONTIUM CONDYLAR GROWTH HORMONAL FACTORS- Command 673/1/2017 99
- 68. GNOMONIC GROWTH & LOGARITHMIC SPIRAL A mathematical model was proposed by Moss that describes mandibular growth along a logarithmic spiral This was based on D’Arcy Thompsons study on sea-shells ( Nautilus) Chambered Nautilus The characteristics of its growth are Original shape remains constant, with increase in size. Gnomonic growth can be described by a curve called as equiangular or logarithmic spiral 683/1/2017 99
- 69. “Gnomon” – that portion or increment which when added doesn’t alter the shape but only produces an increase in size Equiangular or Logarithmic spiral – The growth of the nautilus follows a particular spiral. The important feature of the spiral is movement of point away from pole along the radius vector with velocity increasing with distance from pole The angles formed with pole are equal 693/1/2017 99
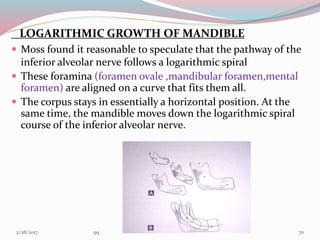
- 70. LOGARITHMIC GROWTH OF MANDIBLE Moss found it reasonable to speculate that the pathway of the inferior alveolar nerve follows a logarithmic spiral These foramina (foramen ovale ,mandibular foramen,mental foramen) are aligned on a curve that fits them all. The corpus stays in essentially a horizontal position. At the same time, the mandible moves down the logarithmic spiral course of the inferior alveolar nerve. 703/1/2017 99
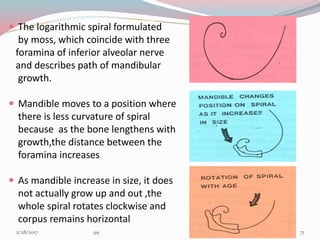
- 71. The logarithmic spiral formulated by moss, which coincide with three foramina of inferior alveolar nerve and describes path of mandibular growth. Mandible moves to a position where there is less curvature of spiral because as the bone lengthens with growth,the distance between the foramina increases As mandible increase in size, it does not actually grow up and out ,the whole spiral rotates clockwise and corpus remains horizontal 713/1/2017 99
- 72. FUNCTIONAL MATRIX THEORY According to the functional Matrix theory Logarithmic growth is related to active and passive processes: Active transformative skeletal growth process occurring at the level of the skeletal units (histologically discernible). Passive translative - primary expansive growth of their capsular functional matrices by an alteration in their spatial position. As the orofacial capsule expands the embedded mandible is passively lowered in space. The capsular matrix expansion is not haphazard but involves postnatal rotation of the inferior alveolar nerve about an axis passing through fixed axis (foramen ovale). 723/1/2017 99
- 73. This suggests that anterior positioning of the mental foramen must be a passive growth event. But the mandibular foramen actively grows up back and out. Hence the distance between the mandibular and mental foramen increases, as does the distance between Ovale and Mandibular foramina. All these increases however are allometric. The position, angulation, resting lengths and tensions of the masseter and medial pterygoid muscles tend to be altered by the passive expansion of the orofacial capsule as a consequence of the rotation of the logarithmic curve. - Neuromuscular adaptation - Neurotrophic regulation 733/1/2017 99
- 74. passive growth of oro-facial capsule primary alterations in resting length contractile and passive tension, and /or angulation of the related muscles change in the growth of the skeletal units alter the muscle activity vectors Active mandibular skeletal growth CNS Membrane conduction Neuromuscular Adaptation 743/1/2017 99
- 75. PROBLEMS OF MANDIBULAR GROWTH AND THEIR ORTHODONTIC SIGNIFICANCE HYPOGNATHISM Agnathia - mandible may be grossly deficient or absent which reflects deficiency of neural crest cell tissue in lower part of the face. First arch and second arch syndrome – Aplasia of mandible and hyoid bone. Micrognathia - a diminutive mandible, occurs in Pierre Robin’s syndrome Cat cry syndrome Mandibulofacial dysostosis Progeria Down’s syndrome Oculo-auriculo vertebral syndrome Turner’s syndrome 753/1/2017 99
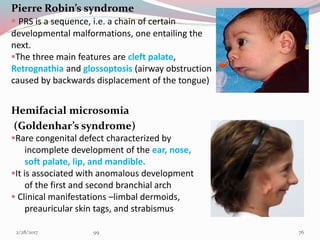
- 76. Pierre Robin’s syndrome PRS is a sequence, i.e. a chain of certain developmental malformations, one entailing the next. The three main features are cleft palate, Retrognathia and glossoptosis (airway obstruction caused by backwards displacement of the tongue) Hemifacial microsomia (Goldenhar’s syndrome) Rare congenital defect characterized by incomplete development of the ear, nose, soft palate, lip, and mandible. It is associated with anomalous development of the first and second branchial arch Clinical manifestations –limbal dermoids, preauricular skin tags, and strabismus 763/1/2017 99
- 77. 773/1/2017 99
- 78. PROGNATHISM Common in males and in conditions like acromegaly Anterior and posterior crossbite will be present Increased mandibular corpus length on ceph Dental and skeletal class III malocclusion TMJ ANKYLOSIS Limited mouth opening Unilateral/bilateral OR Osseous /fibrous Crossbite on affected side Deviation of jaw to affected site while opening Flatness or fullness of affected side 783/1/2017 99
- 79. CONDYLAR HYPERTROPHY Mostly due to genetic or hormonal causes Common in males Usually expressed in late teen age when the growth of mandible continues at condyle More likely to be a high angle case Unilateral-chin divergent on side opposite to hypertrophy facial assymetry buccal crossbite on unaffected side 793/1/2017 99
- 80. EXCESSIVE TRANSVERSE GROWTH Due to genetic reasons Common in prognathic patients Brachiofacial appearance Bilateral crossbite Anterior divergent face In severe cases there can be total lingual non occlusion-Crocodile bite POOR TRANSVERSE GROWTH Common in hypognathic patients Usually class II cases Posterior divergent patients In severe cases there is complete buccal non occlusion-Brodie’s Bite 803/1/2017 99
- 81. PROBLEMS OF RAMAL GROWTH EXCESSIVE VERTICAL RAMAL GROWTH Brachiofacial patients low angle cases anterior deep bite POOR VERTICAL RAMAL GROWTH dolichofacial patients high angle cases anterior open bite EXCESSIVE HORIZONTAL RAMAL GROWTH More broad oropharynx POOR HORIZONTAL RAMAL GROWTH Narrow oropharynx Chances of airway embarassment 813/1/2017 99
- 82. PROBLEMS OF CHIN GROWTH PROMINENT CHIN Common in males Due to late gonial deposition Excessive mental bone resorption Can be treated with genioplasty in adults DEFECTS DUE TO FAILURE OF FUSION OF PROCESSES MANDIBULAR CLEFT; Rare condition due to persistence of furrow between 2 mandibular processes MICROSTOMIA/MACROSTOMIA;Determined by fusion of maxillary and mandibular process at their lateral extent 823/1/2017 99
- 83. SIGNIFICANCE Timely identification of growth disturbances helps in interception of developing malocclusions and other orthodontic and esthetic facial problems Knowing the timing of development of different facial structures gives you idea about the long term facial apppearence of the patient Timely diagnosis of growth problems gives you a chance to treat the problem with functional appliances 833/1/2017 99
- 84. Role of functional appliances in the growth of mandible MANDIBULAR DEFICIENCY A skeletal Class II relationship could be either due to a small mandible or a normal mandible in posterior position. One possibility of treatment is to restrain the growth of maxilla with extra oral force and let the mandible continue to grow more or less normally Enhancement of mandibular skeletal growth and this is done with the help of functional appliance which hold the mandible forward from its retruded position and enhances growth. 843/1/2017 99
- 85. For most mandibular deficient patients: a standard bionator or activator appliance is used as it is a simple, durable and readily acceptable appliance. If transverse expansion is needed ,buccal loops attached to bionator or buccal shields of Frankel appliance shields the cirumoral musculature away and thus helps in transverse expansion Twin block appliance comprising of upper and lower acrylic blocks which works together and helps in positioning lower jaw forward The Herbst appliance ,a fixed functional appliance can also be used to correct class II malocclusion due to retrognathic mandible Mandibular anterior repositioning appliance , Forsus appliance, Cemented twin block can also be used 853/1/2017 99
- 86. MANDIBULAR EXCESS Class III malocclusion because of excessive growth of mandible are extremely difficult to treat. For growth modification, treatment of mandibular excess both functional appliance and chin cup have been used before and throughout the adolescent growth spurt. 1.Class III functional appliance (Bionator) It was designed to rotate the mandible down and back and produce proper occlusal relation by allowing max.posterior teeth to erupt down and forward while restraining eruption of mandibular teeth. 863/1/2017 99
- 87. These appliances also tip the mandibular teeth (incisors) lingually and maxillary incisors facially. 2.Extra oral force: Chin cup treatment Chin cup is attached to head gear for anchorage. Extra oral force directed against the mandibular condyle would restrain growth at that location. Chin cup therapy does accomplish lingual tipping of lower incisors as a result of pressure of the appliance on the lower lip and dentition and a change in direction of mandibular growth, rotating the chin down and back. 873/1/2017 99
- 88. A study was conducted to evaluate the dental and skeletal effects of chin cup using two different force magnitudes Fifty growing class III patients were divided into three groups. Patients in group 1 (n = 20) - 600 g of force per side. Patients in group 2 (n = 20) - 300 g of force per side. Group 3 (n = 10) no treatment was performed Lateral Cephalograms were traced and analyzed before treatment and after one year They concluded that; The use of a chin cup significantly improved the mandibular and maxillary relationship, but with only minor skeletal effects. Reduced ramus height and increased the anterior facial height, mandibular plane angle, and retroclination of the mandibular incisors. Use of 600g force had a more pronounced effect in the reduction of ramus height. Chin cup effects using two different force magnitudes in the management of Class III malocclusions, Yasser L. Abdelnaby and Essam A. Nassar THE ANGLE ORTHODONTIST;SEP.2010 :VOL.8 ,ISS. 5883/1/2017 99
- 89. ENVELOPE OF DISCREPENCY (william R Proffit ,Ackerman J. L) It has three envelopes .The perimeter of each envelope gives the maximum range of movements possible by different methods INNER ENVELOPE- Only orthodontic treatment MIDDLE ENVELOPE- Orthodontic &growth modification OUTERMOST ENVELOPE- Orthodontic & surgical treatment 893/1/2017 99
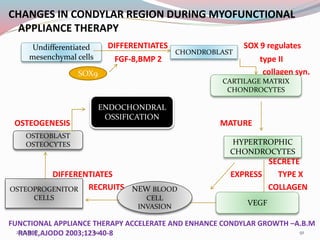
- 91. CHANGES IN CONDYLAR REGION DURING MYOFUNCTIONAL APPLIANCE THERAPY DIFFERENTIATES SOX 9 regulates FGF-8,BMP 2 type II collagen syn. OSTEOGENESIS MATURE SECRETE DIFFERENTIATES EXPRESS TYPE X RECRUITS COLLAGEN FUNCTIONAL APPLIANCE THERAPY ACCELERATE AND ENHANCE CONDYLAR GROWTH –A.B.M RABIE,AJODO 2003;123-40-8 Undifferentiated mesenchymal cells SOX9 CHONDROBLAST CARTILAGE MATRIX CHONDROCYTES HYPERTROPHIC CHONDROCYTES VEGF NEW BLOOD CELL INVASION OSTEOPROGENITOR CELLS OSTEOBLAST OSTEOCYTES ENDOCHONDRAL OSSIFICATION 913/1/2017 99
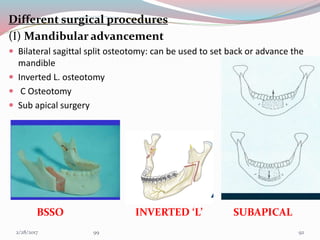
- 92. Different surgical procedures (I) Mandibular advancement Bilateral sagittal split osteotomy: can be used to set back or advance the mandible Inverted L. osteotomy C Osteotomy Sub apical surgery BSSO INVERTED ‘L’ SUBAPICAL 923/1/2017 99
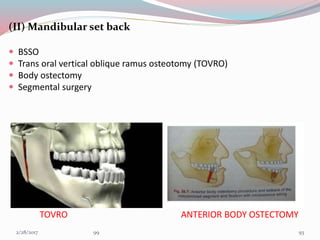
- 93. (II) Mandibular set back BSSO Trans oral vertical oblique ramus osteotomy (TOVRO) Body ostectomy Segmental surgery TOVRO ANTERIOR BODY OSTECTOMY 933/1/2017 99
- 94. Correction of Mandibular Retrognathia and Laterognathia by Distraction Osteogenesis: Follow up of 5 cases-EUR J DENT2009 Oct; 3(4): 335–342. The procedure was carried out in 5 subjects (3 males and 2 females)aged between 14 years and 27 years.3 Patients had undergone bilateral distraction osteogenesis and remaining 2 ,unilateral distrctn.osteogenesis In patients treated with bilateral mandibular distraction, it was observed that the ANB angle decreased by a mean of 5°, the mandibular corpus length increased by a mean of 14.5 mm and the overjet decreased by a mean of 12.2 mm after treatment. In patients treated with unilateral mandibular distraction, a mean of 3.5° reduction was achieved in ANB angle, the mandibular corpus length increased by a mean of 5.5 mm and a mean of 7 mm correction was achieved in relation to craniofacial midline with treatment. It can be concluded that distraction of the deformed mandible is a feasible and effective technique for treating mandibular retrognathia and laterognathia and that long term relapse is within acceptable limits. 943/1/2017 99
- 95. Mandibular Growth, Remodeling, and Maturation During Infancy and Early Childhood(Yi-Ping Liu, Rolf G. Behrents, and Peter H. Buschang) The Angle Orthodontist-vol.80 Jan 2010 In a study lateral cephalograms of 24 females and 24 males, taken between birth and 5 years of age, as well as early adulthood, were traced and digitized. Five measurements and nine landmarks were used to characterize mandibular growth, remodeling, and degree of adult maturity. Ramus height (Co-Go),Overall length (Co-Gn),Corpus length (Go-Gn),Condylion angle (Go-Co-Me),Gonial angle (Co-Go-Me) They concluded that 1. Mandibular size increased 18.2 mm to 34.7 mm between 0.4 and 5.0 years of age. 2. Males displayed greater growth increases for ramus height (Co-Go) than for corpus length (Go-Gn), and females showed similar changes 3. Gonial angle decreased 2.8° and 2.0° in males and females, respectively. 953/1/2017 99
- 96. Regulation of the Response of the Adult Rat Condyle to Intermaxillary Asymmetric Force by the RANKL-OPG System(Yue Xua; Tuojiang Wub; Yangxi Chenc; Zhiguang Zhangd) The Angle Orthod. 2009;79:646–651. The mandibular rami of 160 Sprague-Dawley rats (3 months old) were subjected to unilateral traction in the anterior-superior direction using an elastic force. (120 & 40 g ,then traction removed after28 days. The expression of RANKL and OPG in the subchondral bone of the condyles was analyzed by semiquantitative immunohistochemistry. Results: - Different force levels induced similar changes in the expression of the OPG protein by28 days. -The effect of a 120-g elastic force on the expression of RANKL was stronger than that of a 40-g force. Because of the asynchrony of RANKL responses to external forces of different values, the values of RANKL/OPG ratio showed characteristic variation 963/1/2017 99
- 97. CONCLUSION Bone growth in mandible is a remodelling process represented by apposition and resorption. Knowledge of general facial growth provides a background to the understanding of the etiology and development of of malocclusion, such an understanding is in turn an important part of diagnosis and treatment planning. 973/1/2017 99
- 98. REFERENCES 1.HANDBOOK OF FACIAL GROWTH,SECOND EDTN-ROBERT E MOYERS 2.THE HUMAN FACE-DONALD H ENLOW 3.HUMAN EMBRYOLOGY,EIGHTH EDITION-INDERBIR SINGH 4.ORTHODONTIC CURRENT PRINCIPLES & TECHNIQUE,FIFTH EDITION- T.MGRABER 5.CONTEMPORARY ORTHODONTICS,FIFTH EDITION-WILLIAM R PROFITT 6.DENTOFACIAL ORTHOPEDICS WITH FUNCTIONAL APPLIANCES- GRABER,RAKOSI,PETROVIC 7.CRANIOFACIAL DEVELOPMENT-GEOFFREY H SPERBER 8.PRENATAL DEVELOPMENT OF HUMAN MANDIBLE.THE ANATOMICAL RECORDS 263:314-325(2001) 9.GROWTH OF MANDIBLE DURING PUBESCENCE-ROCHE,LEWIS AO OCT 1982 10.AGE RELATED DIFFERENCE IN RAMUS GROWTH-ENLOW,HANS AJO DEC.1995 . 983/1/2017 99
- 99. 11. VARIATION IN GROWTH PATTERN OF HUMAN MANDIBLE;A LONGITUDINAL RADIOGRAPHIC STUDY BY IMPLANT METHOD- ARNE BJORK ;J DENT RES 1963 12.CORRECTION OF MANDIBULAR RETROGNATHIAAND LATEROGNATHIA BY DISTRACTION OSTEOGENESIS-EUR J DENT 2009 OCT:3(4);335-342 13. MANDIBULAR GROWTH,REMODELLING AND MATURATION DURING INFANCYAND CHILDHOOD-ROLF G BEHRENTS,PETER H BUSCHANG-AO JAN.2010 14.THEORIES OF CRANIOFACIAL GROWTH IN POSTGENOMIC ERA;DAVID S CARLSON: SEM ORTHO ,2005 11:172–183 15. REGULATION OF THE RESPONSE OF THE ADULT RAT CONDYLE TO INTERMAXILLARY ASYMMETRIC FORCE BY THE RANKL-OPG SYSTEM-YUE XUA,TUOIJANG WUB.THE ANGLE ORTHODONTIST 2009;79,646-651 16.FUNCTIONALAPPLIANCE THERAPY ACCELERATE AND ENHANCE CONDYLAR GROWTH –A.B.M RABIE,AJODO 2003;123-40-8 993/1/2017 99