Pathway of Pain
•Download as PPT, PDF•
24 likes•10,141 views

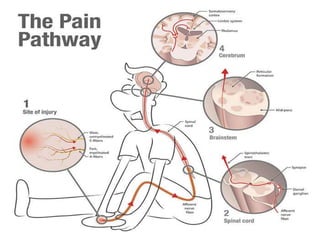
This presentation discusses the pathway of pain from nociception to perception. It begins by defining pain and nociception, describing the characteristics of A-delta and C pain fibers. It then covers the classification of pain and central pain mechanisms, including ascending and descending pathways. Specific types of pain like neuropathic, mixed and idiopathic pain are addressed. Facial pain causes and conditions like trigeminal neuralgia are examined. Finally, visceral pain pathways and various neurological lesions and disorders involving cranial nerves are reviewed.





Pathway of Pain
- 1. 4/5/2014
- 2. 4/5/2014 ‘PATHWAY OF PAIN’ ORAL BIOLOGY PRESENTATION
- 4. 4/5/2014
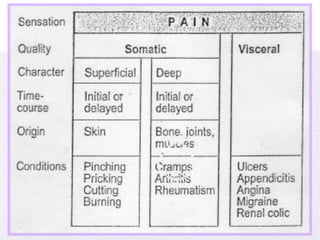
- 5. 4/5/2014 ‘PAIN’ An unpleasant sensory and emotional experience which we primarily associate with tissue damage or describe in terms of such damage, or both.
- 6. 4/5/2014
- 7. 4/5/2014
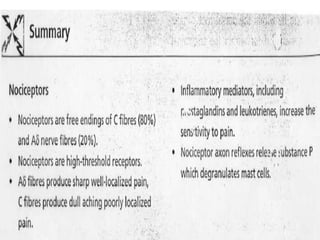
- 8. 4/5/2014 ‘NOCICEPTION’ The detection of tissue damage by specialized transducers connected to A- delta and C-fibers.
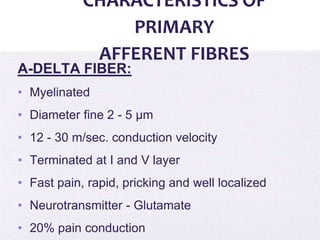
- 9. 4/5/2014 CHARACTERISTICS OF PRIMARY AFFERENT FIBRES A-DELTA FIBER: • Myelinated • Diameter fine 2 - 5 μm • 12 - 30 m/sec. conduction velocity • Terminated at I and V layer • Fast pain, rapid, pricking and well localized • Neurotransmitter - Glutamate • 20% pain conduction
- 10. 4/5/2014 CHARACTERISTICS OF PRIMARY AFFERENT FIBRES C-FIBER: • Non-Myelinated • Diameter less than 2 films • -0.5 to 2 m/s conduction velocity • Terminate in I and n layers • Slow, diffuse, dull, aching
- 11. 4/5/2014 CLASSIFICATION OF PAIN NOCICEPTION • Proportionate to the stimulation of the nociceptor. • When acute •Physiologic pain •Serves a protective function •Normal pain • when chronic •Pathologic pain
- 13. 4/5/2014 NEUROPATHIC PAIN: • Sustained by aberrant processes in PNS or CNS • Disproportionate to the stimulation of nociceptor • Serves no protective function • Pathologic pain
- 14. 4/5/2014 MIXED PAIN: • Nociceptive components • Neuropathic components • Examples: • Failed low-back-surgery syndrome • Complex regional pain syndrome
- 15. 4/5/2014 IDIOPATHIC PAIN: • No underlying lesion found yet, despite investigation • Pain disproportionate to the degree of clinically discernible tissue injury
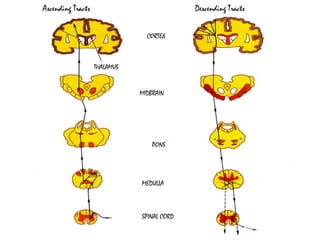
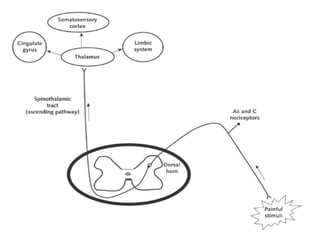
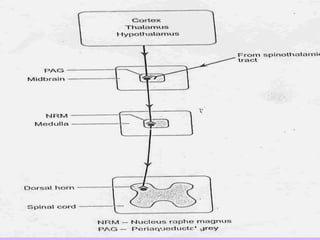
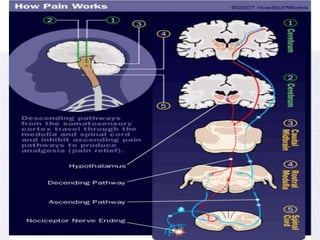
- 17. 4/5/2014 Ascending Tracts Descending Tracts CORTEX MIDBRAIN PONS MEDULLA SPINAL CORD THALAMUS
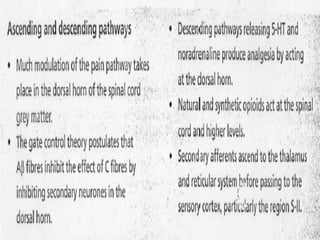
- 18. 4/5/2014 ‘ASCENDING AND DESCENDING PAIN PATHWAYS’
- 19. 4/5/2014
- 20. 4/5/2014
- 21. 4/5/2014 ‘PAIN INHIBITORY AND PAIN FACILITATORY MECHANISMS WITHIN DORSAL HORN’
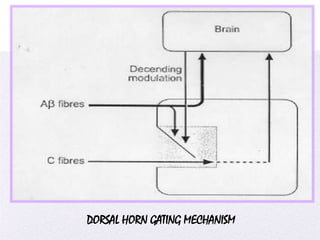
- 22. 4/5/2014 DORSAL HORN GATING MECHANISM
- 23. 4/5/2014 Neuronal circuitry within the dorsal horn. Primary afferent neuron axons synapse onto spinothalmic neurons and onto inhibitory and excitatory neurons.
- 24. 4/5/2014
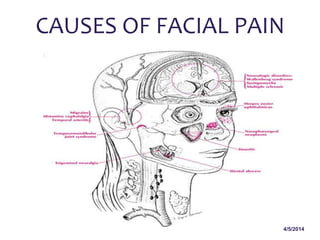
- 26. 4/5/2014 CAUSES OF FACIAL PAIN
- 27. 4/5/2014 CAUSES OF FACIAL PAIN Facial pain can be caused by anything, from an infection to nerve damage in the face. Common causes for facial pain include: • oral infections • ulcers (open sores) • abscess (collection of pus under the surface tissue in the mouth, for example) • skin abscess (collection of pus under the skin) • headache • facial injury • toothache
- 28. 4/5/2014 More serious causes for facial pain include: • herpes zoster (shingles) • migraine • sinusitis (sinus infection) • nerve disorder
- 31. 4/5/2014
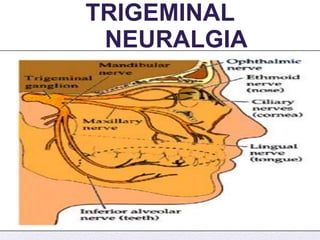
- 32. 4/5/2014 TRIGEMINAL NEURALGIA • Tic douloureux / fothergill’s neuralgia • Paroxysms of fleeting ,excruciating u/l facial pain, usually lasting less than a minute. • Usually V2/V3 , rarely V1 • MC – adv age, women , rt side • Stimulation of trigger zone – pain • Pain – by activities like talking, chewing, brushing teeth, exposure to cold, by wind on face
- 33. 4/5/2014
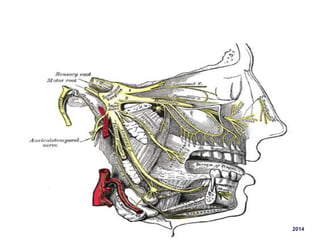
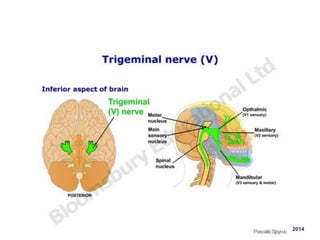
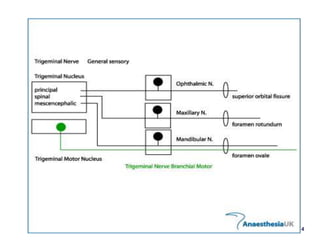
- 34. 4/5/2014 • Trigeminal / gasserian / semilunar ganglion • Situated just beside pons in a shallow depression in petrous apex – meckel’s cave • Sensory root enters the pons course dorsomedially & terminate within brainstem: Nucleus of spinal tract of Vth N Main/Principal sensory nucleus Mesencephalic nucleus
- 35. 4/5/2014 • Fibres – pain & temp – enter spinal tract of trigeminal & descend to various levels depending on their somatotropic origin, then synapse in adjacent nucleus of spinal tract. • The axons of second order neurons cross midline, aggregate as trigeminothalamic tract & ascend to VPM • From VPM , fibres project through thalamic radiations to sensory cortex in post central gyrus
- 36. 4/5/2014
- 37. 4/5/2014 • B/L Weakness of muscles of mastication with inability to close the mouth ( dangling jaw ) – motor neuron ds, neuromuscular transmission disorder, myopathy Clinical examination motor functions
- 38. 4/5/2014 Clinical examination SENSORY FUNCTIONS • Pain, touch, heat, cold – tested on face & mucous membranes • Each of the 3 divisions of Vth.N is tested individually and compared with the opposite side.
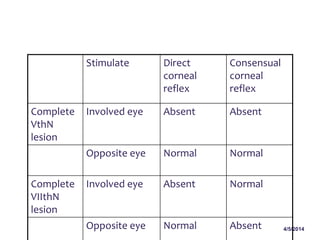
- 39. 4/5/2014 Stimulate Direct corneal reflex Consensual corneal reflex Complete VthN lesion Involved eye Absent Absent Opposite eye Normal Normal Complete VIIthN lesion Involved eye Absent Normal Opposite eye Normal Absent
- 40. 4/5/2014
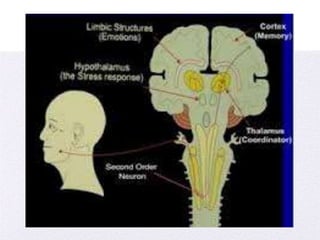
- 41. 4/5/2014 Second-Order Neuron; Some times is called a transmission neuron since it transfer the impulse on to higher center . The synapse of the primary afferent and second-order neuron occurs in the dorsal horn of the spinal cord .
- 42. 4/5/2014 Afferent (Sensory) Somatic Nerves • – Trigeminal Nerve • – Facial Nerve • – Glossopharyngeal Nerve • – Vagus Nerve • – Cervical Spinal Nerves
- 43. 4/5/2014 Efferent (Motor) Somatic Nerves – Occulomotor, and abducent Nerves – Trigeminal Nerve – Facial Nerve – Glossopharyngeal nerve
- 44. 4/5/2014 TYPES OF PAIN • Myofascial Pain • Myositis • Myospasm and Dystonia • Protective Muscle Splinting • Contracture • Neoplasia • Fibromyalgia
- 46. 4/5/2014 Supranuclear lesions • Lesions affecting corticobular pathway - Contralateral trigeminal motor paresis (deviation of jaw away from the lesion) • B/L UMN lesions ( pseudobulbar palsy ) – trigeminal motor paresis , exaggerated jaw jerk.Mastication markedly impaired. • Thalamic lesions – anaesthesia of c/l face • Parietal lesions – depression of c/l corneal reflex
- 47. 4/5/2014 NUCLEAR LEISIONS • Motor , sensory nuclei – primary/met . tumours AV malformations demyelinating ds infarction/h’age syringobulbia that affect pons, medulla and upper cervical cord.
- 48. 4/5/2014 Lesions affecting preganglionic trigeminal nerve roots • Tumour ( meningioma, schwannoma, metastasis, nasopharyngeal ca ) • Infection ( granulomatous, infectious , carcinomatous meningitis ) • Trauma • Aneurysm Char i/p facial pain, parasthesias, numbness, sensory loss, corneal reflex depressed, trigeminal motor paresis.
- 50. 4/5/2014 Lesions affecting peripheral branches of VthCranial Nerve • Ophthalmic div : in middle cranial fossa , at temporal bone apex, lat wall of cavernous sinus, sup.orbital fissure, distally in face • Maxillary div : lower lateral wall of cavernous sinus, at foramen rotundum, in pterygopalatine fossa, in floor of orbit, at infraorbital foramen, in face
- 51. 4/5/2014 Raeder’s paratrigeminal syndrome • U/l oculosympathetic paresis – miosis , ptosis (without facial anhydrosis) • Evidence of trigeminal involvement on same side. • d/t lesions in middle cranial fossa ( b/w trigeminal ganglion & int.carotid.a, near petrous apex) • Lesions of gasserain ganglion – tumour, aneurysm, trauma, infection
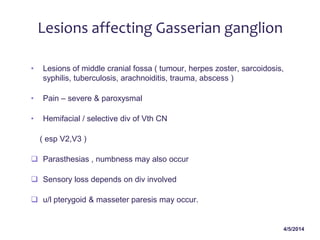
- 52. 4/5/2014 Lesions affecting Gasserian ganglion • Lesions of middle cranial fossa ( tumour, herpes zoster, sarcoidosis, syphilis, tuberculosis, arachnoiditis, trauma, abscess ) • Pain – severe & paroxysmal • Hemifacial / selective div of Vth CN ( esp V2,V3 ) Parasthesias , numbness may also occur Sensory loss depends on div involved u/l pterygoid & masseter paresis may occur.
- 54. 4/5/2014
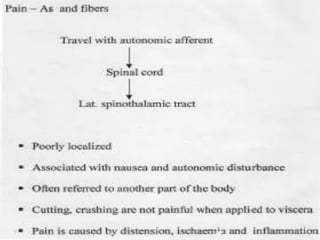
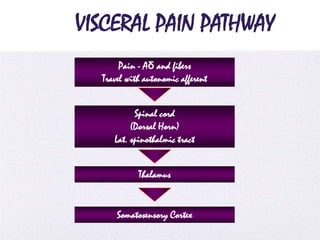
- 55. 4/5/2014 VISCERAL PAIN PATHWAY Pain - Aδ and fibers Travel with autonomic afferent Spinal cord (Dorsal Horn) Lat. spinothalmic tract Thalamus Somatosensory Cortex
- 56. 4/5/2014
- 57. 4/5/2014
- 58. 4/5/2014 ‘REFERENCES’ • Guyton and Hall textbook of Medical Physiology • http://science.howstuffworks.com/life/inside-the-mind/human- brain/pain3.htm • http://www.docstoc.com/docs/ • http://www.google.fr/imgres • www.ksums.net • www.authorstream.com • http://www.docstoc.com/docs/70291468/Pain-Terminology-and-Pain-
- 59. 4/5/2014
- 60. 4/5/2014