Lecture 7 management of head injury patients
- 1. Management of the Head Injury Patient William Schecter, MD
- 2. Epidemilogy • 1.6 million head injury patients in the U.S. annually • 250,000 head injury hospital admissions annually • 60,000 deaths • 70-90,000 permanent disability • Estimated cost: $100 billion per year
- 3. Causes of Brain Injury • Motor Vehicle Accidents • Falls • Anoxic Encephalopathy • Penetrating Trauma • Air Embolus after blast injury • Ischemia • Intracerebral hemorrhage from Htn/aneurysm • Infection • tumor
- 4. Brain Injury • Primary Brain Injury • Secondary Brain Injury
- 5. Primary Brain Injury • Focal Brain Injury – Skull Fracture – Epidural Hematoma – Subdural Hematoma – Subarachnoid Hemorrhage – Intracerebral Hematorma – Cerebral Contusion • Diffuse Axonal Injury
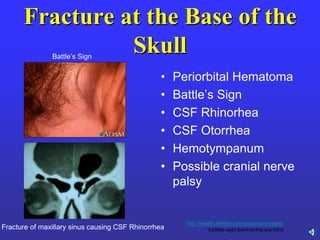
- 6. Fracture at the Base of the Skull • Periorbital Hematoma • Battle’s Sign • CSF Rhinorhea • CSF Otorrhea • Hemotympanum • Possible cranial nerve palsy Fracture of maxillary sinus causing CSF Rhinorrhea Battle’s Sign images/-http://health.allrefer.com/pictures battles-sign-behind-the-ear.html
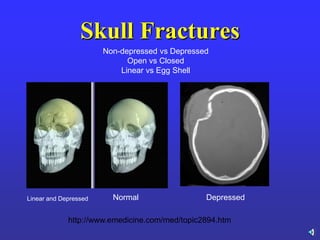
- 7. Skull Fractures Linear and Depressed Normal Depressed Non-depressed vs Depressed Open vs Closed Linear vs Egg Shell http://www.emedicine.com/med/topic2894.htm
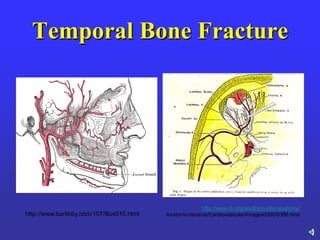
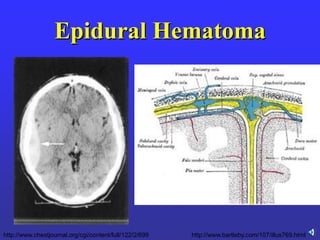
- 10. Epidural Hematoma • Uncommon (<1% of all head injuries, 10% of post traumatic coma patients) • Located between the dura and the skull • Often associated with temporal bone fracture • ―Classic Presentation‖ = Unconsciousness followed by a lucent period followed by deterioration • Look for ipsilateral pupillary dilation
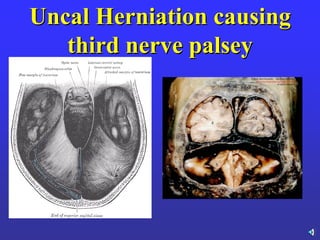
- 11. Uncal Herniation causing third nerve palsey
- 12. Third Nerve Palsy • Constricts pupil • Innervates levator palpebrae of the eyelid • Innervates superior, medial and inferior rectus muscles of eye • Pupillary Dilation • Drooping eyelid Function of Third Nerve Physical Finding
- 13. Third Nerve Palsy • Physical Findings – Dilated Pupil – Drooping Eyelid • Look for Cushing’s Reflex (elevated ICP) – Hypertension – Bradycardia
- 14. Case Presentation • 17 year old girl stuck by a car. Transient loss of consciousness at the scene. Scalp laceration. • Awake and responding in the ER. No CT available. To OR for repair of scalp laceration under local anesthesia. • The next morning speaking in English and Samoan • Drowsey at 16:00 • 16:45: Bilateral dilated pupils and respiratory distress
- 15. Epidural Hematoma •Uncommon (less than 5% of cases) •Classic Findings –Initial Loss of Consciousness –Lucid Interval –Neurological Deterioration •Associated with tear of Middle Meningeal Artery •Prognosis good if timely diagnosis and treatment
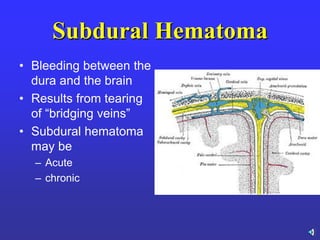
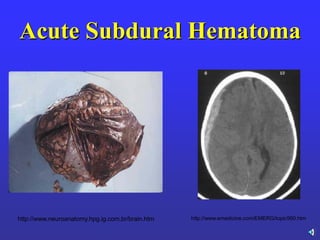
- 16. Subdural Hematoma • Bleeding between the dura and the brain • Results from tearing of ―bridging veins‖ • Subdural hematoma may be – Acute – chronic
- 17. Case Presentation • 35 year old man involved in an automobile accident on a Sunday afternoon at approximately 12:00 noon. Admitted with altered mental status, hemodynamically stable. No major injuries except acute SDH • No neurosurgeon available. Transferred to 2 other hospitals w/o neurosurgeons • 6 hours after accident arrives at San Francisco General Hospital with bilateral fixed and dilated pupils
- 19. Acute Subdural Hematoma •50% Mortality •Return to normal function limited in survivors •More common in older patients •Prevention of Secondary Brain Injury essential
- 20. Case Presentation • 45 year old radiologist arrives for dinner at colleagues’ house for dinner complaining of head ache. Neurological exam normal. • Admitted later in the evening for dizziness. Signs out of hospital AMA the next morning. No CT available. • Returns that afternoon. The next day unconscious with slightly dilated left pupil.
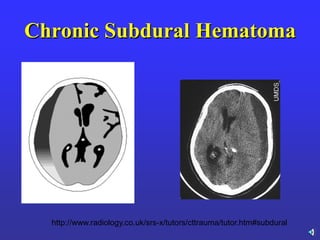
- 22. Chronic Subdural Hematoma •3-6% Mortality Rate •Normal return to neurologic function if diagnosis made early in 65-75% of cases •High index of suspicion in chronic alcoholics, the elderly, patients on anticoagulant therapy
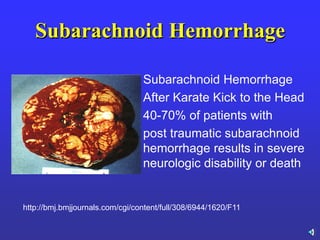
- 23. Subarachnoid Hemorrhage Subarachnoid Hemorrhage After Karate Kick to the Head 40-70% of patients with post traumatic subarachnoid hemorrhage results in severe neurologic disability or death http://bmj.bmjjournals.com/cgi/content/full/308/6944/1620/F11
- 24. Cerebral Contusion • Ipsilateral - Coup • Contralateral – Contrecoup • Clinical Findings depend on location and severity of the contusion • CT Findings – No findings – Localized swelling of the gyri
- 25. Intraparenchymal Hematoma • Similar to CNS mass lesion • Decision to evacuate vs observe difficult
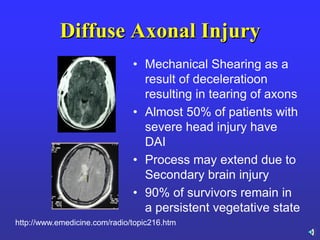
- 26. Diffuse Axonal Injury • Mechanical Shearing as a result of deceleratioon resulting in tearing of axons • Almost 50% of patients with severe head injury have DAI • Process may extend due to Secondary brain injury • 90% of survivors remain in a persistent vegetative state http://www.emedicine.com/radio/topic216.htm
- 27. Primary Brain Injury • Epidural Hematoma • Subdural Hematoma • Subarachnoid Hemorrhage • Cerebral Contusion • Intracerebral Hematoma • Diffuse Axonal InjuryS
- 28. Secondary Brain Injury • Area of original injury extended due to – Cerebral edema – Ischemia – Infection – Herniation
- 29. Goal Prevention of Secondary Brain Injury by Controlling Intracranial Pressure, Maintaining Cerebral Perfusion and Oxygenation
- 30. Cerebral Perfusion Pressure • Adequate CPP essential for prevention of Secondary Brain Injury • CPP = MAP – ICP • CPP should be > 70-80 mm Hg • Systemic Hypotension leads to poor neurological outcome
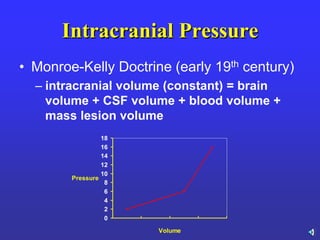
- 31. Intracranial Pressure • Monroe-Kelly Doctrine (early 19th century) – intracranial volume (constant) = brain volume + CSF volume + blood volume + mass lesion volume 0 2 4 6 8 10 12 14 16 18 Volume Pressure
- 32. Signs of increased ICP •Headache •Nausea and vomiting •Change in level of consciousness •Seizures •Change in pattern of ventilation •Papilledema (not after acute trauma) •Change in motor function
- 33. Indications for ICP Monitoring • Severe Head Injury (GCS 3-8) • Moderate Head Injury (GCS 9-12) – Particularly if abnormal CT Scan • Mild Head Injury (GCS 13-15) – little indication for ICP Monitoring
- 34. Methods to Control ICP •Elevate Blood Pressure –Judicious volume expansion –Vasoactive drugs •Hyperventilation—NO!!!!! –Maintain pC02 around 35 mmHg •Diuretics –Mannitol –Use with caution after neurosurgical consultation •Drainage of CSF from Ventriculostomy Catheter
- 35. Maintain CPP • Raise MAP – Volume – Vasopressors • Decrease ICP (if > 20 mm Hg) – Hyperventilation (not recommended) – CSF Drainage – Mannitol (use with caution) 1 gram/kg over 30 minutes
- 36. Management of the Head Injury Patient • Primary Survey – Airway • CERVICAL SPINE CONTROL (5-10% of head injuries associated with cervical spine fracture • Glascow Coma Scale < 8 – indication for intubation – Circulation • Rapidly treat hypotension – Disability • Glascow Coma Scale • Pupils • ? Moves all 4 extremities
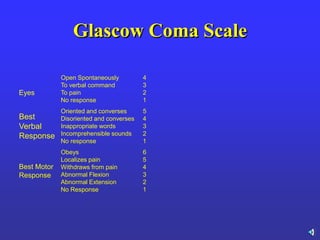
- 37. Glascow Coma Scale 6 5 4 3 2 1 Obeys Localizes pain Withdraws from pain Abnormal Flexion Abnormal Extension No Response Best Motor Response 5 4 3 2 1 Oriented and converses Disoriented and converses Inappropriate words Incomprehensible sounds No response Best Verbal Response 4 3 2 1 Open Spontaneously To verbal command To pain No response Eyes
- 38. Eyes •Open spontaneously – 4 •Open to verbal stimulus – 3 •Open to Pain -- 2 •Unresponsive -- 1
- 39. Verbal Response •Converses appropriately – 5 •Converses but confused – 4 •Speaks only words but not sentences – 3 •Sounds but no words – 2 •No verbal response – 1
- 40. Motor Response •Responds to commands – 6 •Responds to pain with localization – 5 •Responds to pain with withdrawal –4 •Responds to pain with flexion – 3 •Responds to pain with extension – 2 •Unresponsive – 1
- 41. Neurologic Exam during Secondary Survery • (GCS) Mental Status • Cranial Nerve Exam (pupils!!) • Motor Exam of Upper and Lower Extremities • Sensory Exam • Reflexes (Babinski Sign?) • Gait and Station/Ataxia (rarely done in the acute situation
- 42. Potential Abnormalities in Secondary Survey •Hypertension and Bradycardia– Cushing’s Reflex •Cheyne Stokes Respiration in comatose patient-abnormal function of the Medulla Oblongata •Asymmetric pupils—Uncal herniation vs Direct blow to the orbit
- 43. Potential Abnormalities in Secondary Survey •Asymmetric movement of the left vs the right extremities– intracranial mass lesion vs local injury •Asymmetric movement of the upper vs the lower extremities--? Spinal cord injury
- 44. Deterioration in Neurologic Exam? Repeat CT Scan
- 45. Additional Therapy for the Head Injury Patient • Phenytoin 15 mg/kg over 30 minutes with EKG monitor if signs of seizure activity. Prophylactic Treatment to prevent seizures not recommended • Steroids: Not recommended • Barbiturate Coma: In selected cases with uncontrollable Intracranial Hypertension
- 46. Brain Injury • Primary Brain Injury • Secondary Brain Injury
- 47. Primary Brain Injury • Focal Brain Injury – Skull Fracture – Epidural Hematoma – Subdural Hematoma – Subarachnoid Hemorrhage – Intracerebral Hematorma – Cerebral Contusion – Diffuse Axonal Injury • Secondary Brain Injury
- 48. Secondary Brain Injury • Area of original injury extended due to – Cerebral edema – Ischemia – Infection – Herniation
- 49. Goal Prevention of Secondary Brain Injury by Controlling Intracranial Pressure, Maintaining Cerebral Perfusion and Oxygenation