CHAPTER 14 Supracondylar Fractures of the Elbow in Children
INTRODUCTION
Supracondylar humerus fractures are the most common fracture about the elbow in children and have the highest complication rate for elbow fractures in this age group.8,16,39 These compelling facts continue to pique the interest and hold the attention of orthopedists who treat pediatric patients. Since the last edition of this text, issues that have generated the most discussion regarding supracondylar fracture treatment concern timing of reduction and treatment as well as pin configuration used for fracture stabilization. Both issues are addressed in the body of this chapter.
INCIDENCE AND ETIOLOGY
Supracondylar humerus fractures almost exclusively affect the immature skeleton.41,50 Eliason25 reported that 84% of supracondylar fractures occurred in patients younger than 10 years. The peak age for supracondylar humerus fracture has been reported to be between ages 6 and 7 years, and the left arm is injured more frequently than the right.* Previous reports have suggested that supracondylar fractures are common in boys, but more recent studies have documented an equal sex distribution.†
Traditional teaching has held that the peak incidence for extension-type supracondylar humerus fractures occurs at approximately age 7 because that is the age of maximum elbow flexibility and hyperextension. This mechanism has been confirmed by research suggesting that a fall on a hyperextended elbow produces a supracondylar humerus fracture, whereas a fall on an outstretched arm without elbow hyperextension is more likely to cause a distal radius fracture.60 Hyperextension converts what would be an axial loading force to the elbow into a bending moment. The tip of the olecranon acts as a fulcrum, causing the fracture to occur through the relatively thin bone of the olecranon fossa (Fig. 14-1). The distinctive shape of the humeral metaphysis with the medial and lateral condyles and columns, and the narrow midpoint of the olecranon fossa, adds to the instability of the fracture, particularly when there is rotation and tilting of the distal fragment.62,63
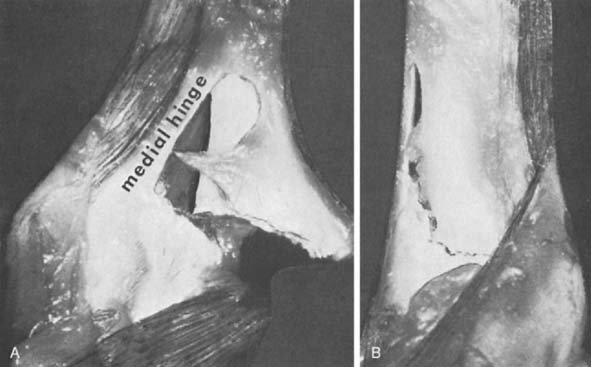
Knowledge of elbow anatomy is important to understanding the cause of the injury, and to understanding effective treatment principles (see Chapters 2 and 3). The stability of the elbow derives from bony and soft tissue structures.33,61,66 Soft tissue stability on the lateral aspect of the elbow is provided by an expansion of the triceps, anconeus, brachioradialis, and extensor carpi radialis longus. The thickened periosteum of a young child, both medially and laterally, is an important additional stabilizer of the fracture fragment and provides a medial or lateral hinge during attempted reduction (Fig. 14-2). Research by Khare et al45 has confirmed the importance of the triceps tendon’s acting as a tension band to achieve fracture stability in the flexed elbow.
Because angular deformity is a common complication of these fractures, the normal variations in pediatric anatomy should be understood. The carrying angle of the elbow joint is the angle formed by the intersection of the longitudinal axis of the arm and the forearm (Fig. 14-3). The normal elbow is usually in slight valgus alignment, but this feature varies among children.1,17,77 Smith77 noted that, of 150 children aged 3 to 11, the carrying angle in boys averaged 5.4 degrees and ranged from 0 to 11 degrees, whereas in girls, it averaged 6 degrees and ranged from 0 to 12 degrees. Aebi1 observed that the measurements were not constant and changed as the child matured, tending to decrease in magnitude and in variation between children.
Although not commonly associated with abuse in the past, a recent report found that 36% of patients younger than age 15 months at the time of their supracondylar fracture sustained the fracture as a result of abuse.79 Clinicians must exclude “nonaccidental trauma” as a potential cause of injury whenever an infant presents with a supracondylar humerus fracture.
CLASSIFICATION
A classification system should guide treatment, provide information on prognosis, and facilitate research by ensuring that similar injuries are compared in the literature. The vast majority of supracondylar humerus fractures can be classified as either flexion or extension injuries, a distinction based on the radiographic appearance and the mechanism of injury. The distinction is important for treatment because the reduction maneuvers are essentially opposite for the two fracture types and flexion-type fractures are significantly more difficult to reduce by closed means. A small minority of fractures exhibit multidirectional instability and do not fit into either flexion or extension types.49 Recognition of multidirectional instability is helpful in formulating an effective treatment strategy.
FLEXION-TYPE FRACTURES
Flexion-type fractures are the result of a direct fall onto a flexed elbow in which a powerful flexion force is applied to the distal humerus, usually through the olecranon. The distal humeral fragment is displaced anteriorly, and the fracture line crosses the humerus from the distal posterior to the proximal anterior aspect (Fig. 14-4). Flexion-type fractures are frequently completely displaced and are difficult to reduce by closed means. The reduction maneuver for flexion-type fractures involves elbow extension or involves using the forearm to apply a posterior-directed force to the anteriorly displaced distal fracture fragment.

EXTENSION-TYPE FRACTURES
Extension-type fractures typically occur as the result of a fall onto an outstretched arm with a hyperextended elbow. The fracture line traverses the distal humerus from the proximal posterior to the distal anterior aspect. Displacement varies from none to marked displacement with fracture fragments separated by interposed soft tissue. Numerous classifications systems have been devised for extension-type supracondylar humerus fractures,10,24,40,41,68 but the classification system attributed to Gartland31 is the most commonly accepted system in use today. As described by Gartland, the classification system is simple, reproducible, helpful in guiding treatment, and provides information on prognosis and potential complications. A very similar fracture classification system was published in the German literature of the early 20th century by Felsenreich.26
TYPE I
Type I fractures are nondisplaced (Fig. 14-5). In many patients, the fracture line may not be visible on injury radiographs, but the posterior fat pad sign, palpable tenderness in the supracondylar region, and an appropriate mechanism of injury allows the physician to establish a correct diagnosis. The diagnosis is often confirmed when periosteal callus is seen on radiographs taken 3 weeks after the injury. If recognized and treated appropriately, type I fractures should never be associated with neurovascular injury or malunion.

TYPE II
In type II fractures, there is displacement or angulation at the fracture site, but a hinge of bone crossing the fracture keeps the fragments in continuity. The distal fragment is most often displaced posteriorly, and apex anterior angulation at the fracture site results in a hyperextension deformity (Fig. 14-6). Variations of type II fractures have also been described that involve medial impaction or rotation, which can result in cubitus varus if unrecognized (Fig. 14-7). Although there are reports of neurovascular injury associated with type II fractures, such injuries are rare.69


TYPE III
Type III fractures are completely displaced fractures in which there is no continuity between fracture fragments (Fig. 14-8). The distal fragment is displaced posteriorly and may be displaced medially or laterally as well. There is a much higher incidence of neurovascular complications with type III fractures, and soft tissue is usually interposed between fracture fragments. The brachialis muscle is most often interposed, but the median nerve, radial nerve, or brachial artery may also be entrapped.

DIAGNOSIS AND RADIOGRAPHIC EVALUATION
We define a supracondylar humerus fracture to be a transverse fracture crossing the entire width of the distal humeral metaphysis without involving the distal humeral physis. The primary challenge in establishing this diagnosis is to rule out other fractures of the distal humerus that do not meet these criteria. Fractures that can sometimes be confused with supracondylar humerus fractures include lateral condyle fractures, medial condyle fractures, and transphyseal fractures. Establishing the correct diagnosis is most difficult in patients younger than 4 years, whose ossific nuclei of the distal humerus are yet unossified.
The anterior and posterior fat pad signs are often helpful in diagnosing intra-articular elbow fractures such as supracondylar humerus fractures (see Chapter 15). Although it is very sensitive, the anterior fat pad sign is not very specific for intra-articular elbow fractures because the coronoid fossa of the humerus (occupied by the anterior fat pad) is much more shallow than the olecranon fossa (occupied by the posterior fat pad). Any insult that causes a joint effusion may cause the anterior fat pad to become visible on the lateral radiograph. A larger intra-articular fluid collection such as fracture hemarthrosis is necessary to displace the posterior fat pad enough for it to become visible on lateral radiographs; therefore, the posterior fat pad sign is much more reliable.
Additional radiographic measurements have been described to assess fracture alignment before and after reduction. The most commonly used measurement is Baumann’s angle, the intersection of a line drawn along the longitudinal axis of the humerus and a line drawn along the physis between capitellum and distal lateral humeral metaphysis. The normal angle varies in magnitude but averages approximately 72 degrees, and it should always be compared with the uninjured contralateral elbow (Fig. 14-9).88 A second useful radiographic reference line is the anterior humeral line (Fig. 14-10). If the capitellar ossific nucleus is displaced posterior to the anterior humeral line, fracture reduction should be considered. Fracture reduction should restore Baumann’s angle to a measurement similar to that of the opposite elbow on the anteroposterior view, and on the lateral view, it should restore the capitellum to a position in which the central third is bisected by the anterior humeral line.

For all patients with supracondylar humerus fractures, the entire extremity should be examined and radiographs obtained of all areas where associated injuries might be present. Approximately 15% of patients with supracondylar fractures have an associated fracture in the ipsilateral extremity.86 Supracondylar fracture associated with a Montaggia lesion has also been reported.3,65
TREATMENT
TYPE II FRACTURES
Despite an intact osseous hinge, type II fractures can vary significantly in displacement and injury severity, which determines treatment choice. For fractures in which the anterior humeral line does intersect the capitellum, reduction may not be necessary and immediate cast immobilization in 90 degrees of flexion is appropriate. Closed reduction should be seriously considered for moderately displaced fractures when the anterior humeral line passes anterior to the capitellum. In a cooperative reliable patient with minimal elbow swelling, gentle closed reduction may be performed under regional anesthesia or conscious sedation in the emergency department, and the fracture should be immobilized in an above-elbow cast with enough flexion to maintain fracture reduction (see Fig. 14-6). If any swelling is present, close attention to the neurovascular examination is critical when immobilizing the elbow in more than 100 degrees of flexion. Fluoroscopic obser-vation can be helpful in determining the minimum degree of flexion required to safely maintain fracture reduction.






