

Abstract
Objective Electronic health records (EHRs) have become widely adopted with increasing emphasis on improving care delivery. Improvements in surgery may be limited by specialty-specific issues that impact EHR usability and engagement. Accordingly, we examined EHR use and perceptions in urology, a diverse surgical specialty.
Methods We conducted a national, sequential explanatory mixed methods study. Through the 2019 American Urological Association Census, we surveyed urologic surgeons on EHR use and perceptions and then identified associated characteristics through bivariable and multivariable analyses. Using purposeful sampling, we interviewed 25 urologists and applied coding-based thematic analysis, which was then integrated with survey findings.
Results Among 2,159 practicing urologic surgeons, 2,081 (96.4%) reported using an EHR. In the weighted sample ( n = 12,366), over 90% used the EHR for charting, viewing results, and order entry with most using information exchange functions (59.0–79.6%). In contrast, only 35.8% felt the EHR increases clinical efficiency, whereas 43.1% agreed it improves patient care, which related thematically to information management, administrative burden, patient safety, and patient–surgeon interaction. Quantitatively and qualitatively, use and perceptions differed by years in practice and practice type with more use and better perceptions among more recent entrants into the urologic workforce and those in academic/multispecialty practices, who may have earlier EHR exposure, better infrastructure, and more support.
Conclusion Despite wide and substantive usage, EHRs engender mixed feelings, especially among longer-practicing surgeons and those in lower-resourced settings (e.g., smaller and private practices). Beyond reducing administrative burden and simplifying information management, efforts to improve care delivery through the EHR should focus on surgeon engagement, particularly in the community, to boost implementation and user experience.
Keywords: electronic health records, satisfaction, usability, user experience, practice setting
Background and Significance
Surgery accounts for a vast swath of health care services. In 2014, 14.1 million inpatient procedures were performed in the United States, accounting for 28.6% of all hospitalizations. 1 In 2019, 15.7 million ambulatory procedures occurred in hospital-owned facilities with additional procedures performed in physician-owned centers. 2 Although most patients recover well, these procedures can generate significant morbidity and cost. As many as 5% of outpatient surgeries result in unplanned hospital visits. 3 Meanwhile, 10% of patients undergoing major inpatient surgery are readmitted. 4 In total, surgery accounts for 50% of Medicare expenditures. 5
In 2009, the Health Information Technology for Economic and Clinical Health Act promoted the adoption and meaningful use of health information technology (IT). 6 Since then, the adoption of electronic health records (EHRs) has increased dramatically. 7 8 9 Now that EHRs have become widespread, attention has shifted toward leveraging the EHR to improve health care delivery. Already, hospitals use EHR data to guide care delivery, particularly for quality improvement and patient safety. 10 Yet, the EHR's impact on outcomes has been mixed with growing recognition that EHR-based tools and interventions need to be more user-centered to facilitate implementation and effectiveness. 11 12 13 14 Most of this work has focused on primary care or medical physicians. However, surgeons and surgical care are inherently different as they are more episode and procedure based. Prior studies have characterized differences in EHR adoption among nonsurgical and surgical specialties and differences in time and usage patterns. 9 15 16 17 18 19 20 21 22 23 Very few though have investigated surgeon perceptions of the EHR or the underlying reasons (e.g., clinical practice, culture) for their experience. 24 25
Objective
Therefore, efforts to improve quality and efficiency in surgery through the EHR require greater contextual detail. Accordingly, we conducted a mixed methods study in urology—a diverse surgical specialty that covers the breadth of modern surgical care (e.g., office-based, endoscopy, ambulatory, minimally invasive, and open surgery)—to characterize current usage patterns and uncover underlying perceptions. This information may inform more usable and useful EHR-based tools to improve care in surgery.
Methods
Study and Survey Design
To assess the use and perceptions of the EHR, we performed a sequential explanatory mixed methods study that connected and integrated a national survey with qualitative interviews from practicing urologic surgeons. 26 The national survey was administered through the 2019 American Urological Association (AUA) Census from May to September 2019 followed by qualitative interviews conducted from June to July 2020. The AUA Census is a large-scale, electronic survey of the urologic workforce conducted annually. It encompasses core questions on demographics (e.g., gender, race/ethnicity, and geography), training/experience (e.g., specialty/subspecialty, years in practice, and fellowship), and clinical practice (e.g., practice type/size, ownership, patient volume, major inpatient cases, and work effort), and it provides sampling weights for national estimates. The AUA Census begins with onsite administration at the AUA Annual Meeting followed by email invitations every 4 to 6 weeks. Token incentives (e.g., t-shirts and raffle items) are given to promote participation.
In the 2019 AUA Census, practicing urologic surgeons reporting the use of an EHR completed supplemental questions on EHR use and perceptions adapted from the National EHR survey. The National EHR Survey is conducted annually by the National Center for Health Statistics on behalf of the Office of the National Coordinator for Health Information Technology and has been shown to have content validity through cognitive interviewing. 18 Respondents were asked to select which of nine specific EHR functions they use “regularly” ( Fig. 1 ) and were also provided an open text field to add additional functions. On a 5-point Likert scale (1: strongly disagree to 5: strongly agree), respondents also rated their agreement with two statements: (1) using the EHR increases clinical efficiency and (2) the EHR helps me deliver better patient care.
Fig. 1.
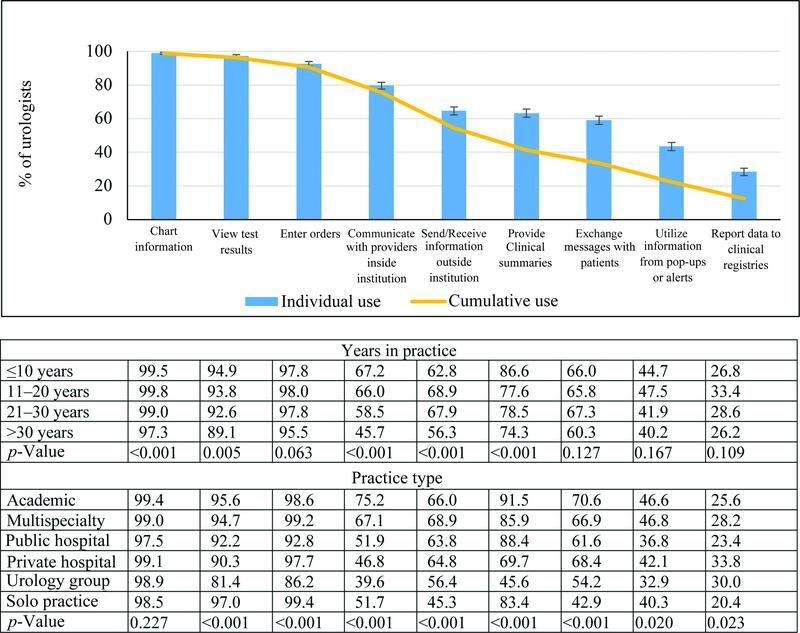
Routine use of EHR functions—individual and cumulative. Figure displays the percent reporting routine use of individual EHR functions. Cumulative use is the percent using the individual function and preceding ones. Tables report use by years in practice and practice type. Population estimates and 95% confidence intervals generated from sampling weights based on gender, geographic location, certification status, and years since initial certification.
Connection and Qualitative Interviews
Building upon the survey, we developed an interview guide based on conceptual frameworks in medical decision-making, clinical informatics, and implementation science to explore two primary topic areas: (1) surgical decision-making and (2) EHR-based clinical decision support ( https://www.med.unc.edu/urology/wp-content/uploads/sites/637/2022/12/Interview-Guide.pdf ). The interview guide was iteratively refined through two pilot interviews to ensure that it would elicit detail and insight from participants in the allotted time. Specific to the EHR, participants were asked about their experiences with the EHR and the effects on clinical efficiency and patient care. Trained qualitative researchers with extensive experience facilitating conversations with health care stakeholders conducted the interviews.
Among AUA Census respondents who consented to follow-up contact (62.9%), we completed 25 qualitative interviews by telephone, each lasting approximately 45 minutes. Participants provided verbal informed consent and received a $100 gift card upon completion. An unadjusted analysis of the survey data indicated relationships between EHR use/perceptions and years in practice and weekly patient encounters. Connecting these preliminary results, we randomly sampled urologists based on these attributes (<18 vs. 18+ years in practice, <75 vs. 75+ patient encounters/week). Nearing theme saturation by interview 18, we then purposively sampled urologists with negative attitudes to capture diverse views with secondary consideration given to gender, geography, and practice type. By interview 25, the qualitative interviewers no longer elicited new information, indicating theme saturation.
Data Analysis and Integration
For the survey questions, a standard poststratification weighting technique was applied based on gender, geographic location, certification status, and years since initial certification to generate summary statistics. For clinical efficiency and patient care, we created a net favorability rating defined as the difference between the proportion agreeing minus the proportion disagreeing. Next, we created binary measures for EHR use (above the median number of functions vs. not), clinical efficiency (strongly agree/agree vs. not), and patient care (strongly agree/agree vs. not). For each outcome, we performed bivariable analysis with chi-squared testing and built multivariable logistic regression models to identify relating characteristics. Covariates included years in practice, gender, race (white vs. nonwhite), fellowship training, AUA section, rurality, scope of practice (general vs. subspeciality), practice setting (solo, urology group, multispecialty, private hospital, academic medical center, public, and other), ownership status, practice size, patient encounters/week, minutes/visit, major inpatient cases/month, clinical hours/week, and nonclinical hours/week.
All interviews were recorded, transcribed, and deidentified. Transcripts were imported into Dedoose, a qualitative research software management tool, to facilitate analysis. Based on the interview guide and field notes, we developed a codebook and then pilot tested it by independently coding several transcripts, which led to fine-tuning concept definitions and revising decision rules. The research team then applied the resulting codebook ( https://www.med.unc.edu/urology/wp-content/uploads/sites/637/2022/12/ACS-Codebook.pdf ) to the remaining interview transcripts, capturing emerging themes and reconciling discrepancies through discussion and consensus. Standard consensus coding procedures were followed. 27 The study team generated code reports for each code and crafted narrative summaries describing themes and subthemes along with illustrative quotes. Finally, we integrated quantitative and qualitative findings to gain deeper insight into EHR use and perceptions. This was completed iteratively through the use of a weaving narrative and joint displays linking survey responses to qualitative themes. This analysis focuses on codes and themes specific to the EHR.
This study received approval from the UNC Institutional Review Board (IRB# 18-3166). The survey questions underwent additional clearance through AUA statistical services. Statistical analyses were performed using SAS v9.4 (Cary, NC) with significance set at the 0.05 level.
Results
Electronic Health Records Usage
In total, 2,081 of 2,159 (96.4%) practicing urologic surgeons completing the AUA Census reported using an EHR and completed the supplemental questions (weighted sample n = 12,366). Characteristics of survey respondents and interview participants are reported in Table 1 . Fig. 1 depicts the use of EHR functions. Nationally, urologic surgeons used a median of six functions (95% CI = 5.8–6.1) with 90.6% (95% CI = 89.0–91.2%) using the EHR for charting, reviewing results, and order entry. Most urologic surgeons made use of information exchange functions, ranging from 59.0% (95% CI = 56.6–61.5%) for exchanging messages with patients to 79.6% (95% CI = 77.6–81.6%) for communicating with health care providers internally, though this varied with years in practice and practice type ( Fig. 1 ). Less than half regularly made use of pop-up alerts (43.4%, 95% CI = 41.0–45.9%) or reported data to clinical registries (28.4%, 95% CI = 26.2–30.5%). Additional functions reported include billing, scheduling, research/quality improvement, and clinical reminders.
Table 1. Characteristics of survey respondents and interview participants.
| Covariate | Level | Surveys ( N = 12,366) | Interviews ( N = 25) |
|---|---|---|---|
| Years in practice, median (interquartile range) | 19.4 (7.7–32.0) | 15 (6-21) | |
| Gender | Male | 89.7% (88.4–91.1) | 64% |
| Female | 10.3% (8.9–11.7) | 36% | |
| Race | White | 79.4% (77.4–81.4) | 80% |
| All other races | 20.7% (18.7–22.7) | 20% | |
| AUA section | North Central | 18.6% (16.7–20.6) | 16% |
| South Central | 14.0% (12.3–15.7) | 4% | |
| Mid-Atlantic | 10.2% (8.7–11.7) | 20% | |
| Northeastern | 3.7% (2.8–4.5) | 8% | |
| New England | 5.7% (4.6–6.7) | 4% | |
| Western | 18.8% (16.8–20.7) | 16% | |
| Southeast | 21.3% (19.4–23.3) | 32% | |
| New York | 7.8% (6.4–9.2) | 0% | |
| Fellowship | Yes | 39.5% (37.1–41.8) | 56% |
| No | 60.5% (58.2–62.9) | 44% | |
| Clinical scope | General | 58.3% (55.9–60.7) | 48% |
| Subspecialty | 41.7% (39.3–44.1) | 52% | |
| Rurality | Metro | 90.0% (88.5–91.5) | 92% |
| Rural | 10.0% (8.5–11.5) | 8% | |
| Ownership | Employed | 61.7% (59.3–64.1) | 72% |
| Any | 38.3% (36.0–40.7) | 28% | |
| Practice type | Academic | 28.7% (26.5–30.9) | 36% |
| Multispecialty | 14.4% (12.8–16.1) | 12% | |
| Private hospital | 8.0% (6.6–9.4) | 8% | |
| Urology group | 30.0% (27.8–32.2) | 20% | |
| Solo practice | 7.0% (5.6–8.3) | 8% | |
| Public | 8.6% (7.1–10.0) | 8% | |
| Other | 3.4% (2.5–4.4) | 8% | |
| Practice size, median (interquartile range) | 6.1 (2.3–14.5) | 10 (3–29) | |
| Major inpatient cases/month, median (interquartile range) | 4.5 (1.3–9.6) | 6 (3–16) | |
| Patient encounters/week, median (interquartile range) | 69.5 (48.6–99.1) | 70 (40–90) | |
| Minutes/visit, median (interquartile range) | 14.6 (11.3–19.3) | 15 (10–20) | |
| Clinical hours/week, median (interquartile range) | 49.1 (35.0–59.2) | 45 (35–60) | |
| Nonclinical hours/week, median (interquartile range) | 4.9 (1.8–9.9) | 10 (4–20) | |
| Joint Display 1: perceptions of the EHR | |||
|---|---|---|---|
| Survey question | Survey response | % (95% CI) | Qualitative themes and exemplar quotes |
| Improve clinical efficiency | Strongly agree | 13.3 (11.6–15.0) | Information management–access to data “You can see records from a long time ago, and so I think that's a positive of electronic health records. We have it all there at our fingertips. I can see more records from outside hospitals, which is also great.” Information management–information overload “The other problem is you've got like 1,000 notes. You can't read all thousand notes. You got to figure out where is the information that you actually require in here. That can be really difficult to find.” Administrative burden “ I spend way too much time [on] unimportant things. If it won't affect my clinical management or recommendation, it won't affect the medical care of that patient that I have to spend time either after hours, between patients, making sure that my computer chart is correct.” |
| Agree | 22.5 (20.5–24.6) | ||
| Neutral | 16.8 (15.0–18.6) | ||
| Disagree | 22.2 (20.2–24.2) | ||
| Strongly disagree | 25.2 (23.1–27.4) | ||
| Better patient care | Strongly agree | 15.2 (13.4–16.9) | Patient safety “I hate it, but then again, the occasional pop-up that says, 'Oh, this patient is deathly allergic to the drug you're trying to write for 'em.' It's like, I'm glad I got this electronic policeman here. It has its benefits.” (Not) practicing at top of license “It dummies down the providers a bit. You want everybody to work at their highest level, and I think that physicians were lowered...We're answering emails. We're looking at inboxes…We didn't go to medical school to click boxes.” Patient-provider interaction “I know a lot of people are doing their notes while they talk to the patients, but I think it distracts from your attention to them…I hear so many patients complain, 'Oh, my gosh. He doesn't even look up anymore,'…I think it takes a little bit away from the interaction.” |
| Agree | 27.9 (25.7–30.1) | ||
| Neutral | 23.5 (21.4–25.6) | ||
| Disagree | 17.5 (15.6–19.4) | ||
| Strongly disagree | 15.9 (14.1–17.6) | ||
Abbreviations: AUA, American Urological Association; CI, confidence interval; EHR, electronic health record; OR, odds ratio.
Electronic Health Record Impact on Clinical Efficiency
Joint Display 1 conveys the reported impact of the EHR on clinical care alongside qualitative themes and exemplar quotes. Overall, 35.8% (95% CI = 33.5–38.2%) of urologic surgeons agreed that using the EHR increases clinical efficiency, while 47.4% (95% CI = 45.0–49.9%) disagreed, resulting in a negative net favorability rating of −11.6%. Qualitatively, interview participants focused on information management (access to data vs. information overload) and administrative burden. The EHR enables greater access to data (e.g., notes, results, and medications) across different encounters and providers and through interoperability (e.g., data from external settings) that facilitates information gathering. Additionally, participants voiced appreciation for enhanced connectivity (e.g., at home and mobile device) that allows for more timely and convenient access with reduced effort.
“Now it's very efficient…On the phone, I can do most things, look at x-rays from the ER, things like that. It's really saved me a lot of time.”
However, the expanded, templated, and often redundant documentation to meet billing requirements can result in information overload that renders the EHR incoherent and cumbersome to use. Participants described a “sea of superfluous” documentation arising from pages of copied information. As an additional subtheme, participants highlighted the nonintuitive design of the EHR that further exacerbates this problem.
“I feel like I could be far more efficient if I could just do it on paper in a simpler format… Every EHR I've ever used organizes things in a nonintuitive way… you're having to navigate through all these screens to try to find the last message or the last lab result.”
Furthermore, participants described an overarching sense of administrative burden. Participants referenced the innumerable, clerical tasks that slow each clinical encounter and negate other efficiency gains. In addition to the voluminous documentation and nonintuitive design, participants listed closing encounters, scheduling visits, applying codes, managing inboxes, answering messages, clicking boxes, and toggling tabs that require extra effort and time. As one participant voiced, “I'm not an Epic-input specialist. I'm a physician.”
Electronic Health Record Impact on Patient Care
In contrast, more urologic surgeons agreed (43.1% [95% CI = 40.6–45.5%]) that the EHR helps them deliver better patient care than disagreed (33.4% [95% CI = 31.1–35.7%]) with a positive net favorability of +9.7%. As reported in Joint Display 1 , this positive outlook relates qualitatively to patient safety and the avoidance of adverse events due to systems within the EHR. Participants also highlighted the benefit of having more complete information when providing recommendations or treatment. Despite these benefits, participants found poor information management to be harmful, citing how excessive and disorganized documentation can lead to missed or incorrect information and worse patient care.
“On some level, [it's] good. When I write prescriptions, it all goes through Epic. It automatically checks my prescriptions against everything else they have…It lets me see things from other doctors' offices. In the old days, somebody would be treating something for one thing. You'd be treating for another. You'd never know that you were having this issue or crossing over. The flip side is there's so much information that sometimes it's hard to pull out the important stuff…because of that people can miss things.”
Related to administrative burden, participants voiced frustration over how the EHR prevents them from “practicing at the top of license” and interferes with patient-provider interactions. Compared to pre-EHR, participants spent much more time performing tasks that could be completed by other staff. As a result, some expressed a sense of “lowering” with less time to practice medicine. At a more basic level, participants described significant disruptions in their interactions with patients and voiced concerns about how this affects patient perceptions, rapport, and trust. As one participant noted, “we treat the chart more than the patient.”
Factors Influencing Electronic Health Record Use and Perceptions
Finally, EHR use and perceptions varied by several factors. Table 2 reports the results from the multivariable analyses. Use and perceptions differed significantly based on practice setting (e.g., type, size, and location) with years in practice as a significant determinant for clinical efficiency and patient care. Joint Display 2 stratifies net favorability ratings by these factors superimposed with related themes. More recent surgeons rated the EHR more favorably, explaining how the EHR was part and parcel of their medical training. Several used multiple different systems from the beginning of their training so felt less daunted and more prepared for using and optimizing the EHR for practice. In contrast, participants with more years in practice described a steep “learning curve” with feelings ranging from excitement to resignation.
Table 2. Respondent characteristics and EHR use and perceptions (multivariable regression results).
| Seven or more EHR functions | Improve clinical efficiency | Better patient care | |||||
|---|---|---|---|---|---|---|---|
| Variable | OR (95% CI) | p -Value | OR (95% CI) | p -Value | OR (95% CI) | p -Value | |
| Years in practice (5-y increments) | 0.96 (0.92–1.00) | 0.065 | 0.94 (0.89–0.98) | 0.005 | 0.92 (0.88–0.96) | <0.001 | |
| Gender—female | 1.05 (0.75–1.47) | 0.768 | 0.91 (0.65–1.27) | 0.559 | 0.99 (0.71–1.38) | 0.935 | |
| Race—all other races | 1.02 (0.79–1.32) | 0.880 | 1.43 (1.10–1.86) | 0.007 | 1.27 (0.98–1.64) | 0.066 | |
| AUA section | North Central | 1.29 (0.93–1.79) | 0.122 | 1.25 (0.89–1.78) | 0.201 | 1.66 (1.20–2.32) | 0.003 |
| South Central | 1.29 (0.91–1.82) | 0.155 | 1.34 (0.94–1.91) | 0.833 | 1.30 (0.92–1.84) | 0.136 | |
| Mid Atlantic | 1.46 (0.99–2.15) | 0.056 | 1.66 (1.11–2.49) | 0.014 | 1.71 (1.15–2.54) | 0.008 | |
| Northeastern | 1.02 (0.60–1.74) | 0.934 | 1.20 (0.69–2.08) | 0.519 | 1.40 (0.81–2.41) | 0.231 | |
| New England | 1.49 (0.93–2.40) | 0.096 | 1.78 (1.12–2.84) | 0.015 | 1.21 (0.76–1.90) | 0.422 | |
| Western | 1.34 (0.97–1.87) | 0.078 | 1.23 (0.88–1.73) | 0.230 | 1.47 (1.06–2.05) | 0.022 | |
| Southeast | Ref | Ref | Ref | ||||
| New York | 0.59 (0.37–0.95) | 0.029 | 1.81 (1.15–2.83) | 0.010 | 1.39 (0.89–2.17) | 0.151 | |
| Fellowship—yes | 0.95 (0.70–1.28) | 0.721 | 1.25 (0.91–1.71) | 0.173 | 1.01 (0.74–1.36) | 0.973 | |
| Clinical scope—subspecialty | 1.15 (0.83–1.60) | 0.402 | 0.73 (0.53–1.01) | 0.060 | 1.03 (0.75–1.41) | 0.866 | |
| Rurality—rural | 1.02 (0.71–1.47) | 0.917 | 1.57 (1.04–2.36) | 0.030 | 1.36 (0.93–2.00) | 0.113 | |
| Ownership—any | 0.73 (0.56–0.97) | 0.027 | 0.98 (0.74–1.29) | 0.877 | 0.82 (0.62–1.08) | 0.150 | |
| Type | Academic | 1.56 (1.07–2.28) | 0.021 | 1.17 (0.80–1.71) | 0.414 | 1.48 (1.01–2.16) | 0.044 |
| Multispecialty | 1.80 (1.28–2.52) | <0.001 | 1.21 (0.86–1.71) | 0.277 | 1.48 (1.06–2.07) | 0.021 | |
| Private hospital | 1.18 (0.74–1.88) | 0.478 | 1.03 (0.62–1.72) | 0.902 | 1.05 (0.65–1.71) | 0.841 | |
| Urology group | Ref. | Ref. | Ref. | ||||
| Solo practice | 0.99 (0.58–1.69) | 0.978 | 1.53 (0.92–2.57) | 0.104 | 1.47 (0.88–2.45) | 0.141 | |
| Public | 0.75 (0.47–1.20) | 0.237 | 1.55 (0.95–2.51) | 0.078 | 1.58 (0.98–2.56) | 0.061 | |
| Other | 1.81 (1.00–3.29) | 0.125 | 1.97 (1.06–3.67) | 0.033 | 2.07 (1.13–3.80) | 0.019 | |
| Practice size | 1.02 (1.01–1.03) | <0.001 | 1.01 (1.00–1.02) | 0.071 | 1.01 (1.00–1.02) | 0.019 | |
| Major inpatient cases/month | 1.00 (0.99–1.02) | 0.551 | 1.01 (1.00–1.02) | 0.152 | 0.99 (0.98–1.01) | 0.278 | |
| Patients encounters/week | 1.00 (1.00–1.01) | 0.072 | 1.00 (1.00–1.00) | 0.685 | 1.00 (1.00–1.00) | 0.924 | |
| Minutes/visit | 1.01 (0.99–1.02) | 0.621 | 1.01 (0.99–1.03) | 0.204 | 1.01 (1.00–1.03) | 0.157 | |
| Clinical hours/week | 1.01 (1.00–1.01) | 0.055 | 0.99 (0.99–1.00) | 0.006 | 1.00 (0.99–1.00) | 0.397 | |
| Nonclinical hours/week | 1.00 (0.99–1.01) | 0.945 | 0.99 (0.98–1.00) | 0.101 | 0.99 (0.98–1.00) | 0.140 | |
| Joint Display 2—EHR perceptions by key characteristics | ||||
|---|---|---|---|---|
| Key characteristics | Perceived impact a (quantitative) | Themes with exemplar quotes (qualitative) | ||
| Clinical efficiency | Patient care | |||
| Overall | −11.6% | +9.7% | ||
| Years in practice | ≤10 | +7.5% | +29.9% | EHR exposure/adoption Early exposure: “ VA had one EHR, clinical setting had Epic, [hospital] had Cerner. To me, I've always had to use a bunch. I'm not stressed out about it. My partners hate it. All the younger ones can handle…” Later adoption: “I'd just say I remember when EHRs first came out, there was a little bit of pushback. I mean, there were docs who refused…and they would fight it for years and years, and they got left behind” |
| 11–20 | −11.2% | +12.3% | ||
| 21–30 | −28.0% | −7.5% | ||
| >30 | −20.8% | −1.8% | ||
| Practice size | <5 | −16.4% | +0.3% | Infrastructure Fragmented: “In the office, we use UroChart. Two hospitals, Epic, then one is Cerner or PowerChart or something like that. It would be really nice if I could use at least one of my hospital's EHRs.” Integrated: “I think it's a dramatic improvement. We literally had seven computer systems we had to go through. It was a nightmare trying to coordinate all that stuff. At least everything's collated in one system now.” Support External support: “Epic requires the use of scribes in our clinics. I would say it's significantly decreased our efficiency and increased our overhead...If it was stand-alone, we would never use that product. It's just not cost-effective for a private practice.” System optimization: “What I do use is a lot of templates. My documentation and order sets are so well fine-tuned that I really have very minimal to fill in…It's just a lot of simple things to prompt myself through, so my documentation time is very quick because of that.” |
| ≥5 | −8.6% | +15.5% | ||
| Practice type | Academic | −9.5% | +22.7% | |
| Multispecialty | −6.5% | +16.0% | ||
| Public | −2.4% | +20.6% | ||
| Private hospital | −18.7% | −0.1% | ||
| Urology group | −19.7% | −5.5% | ||
| Solo practice | −11.2% | −4.7% | ||
| Rurality | Urban | −9.2% | +11.8% | |
| Rural | −33.1% | −9.4% | ||
Abbreviations: AUA, American Urological Association; CI, confidence interval; EHR, electronic health record; OR, odds ratio.
EHR use and perceptions also differed between larger, more integrated, higher-resourced systems (e.g., academic, multispecialty groups, and public and private systems) and smaller, private practices, due likely to infrastructure and support. Some participants described their use of multiple and separate EHR systems, operational differences between systems, and the inefficiency this fragmentation brings compared to a single EHR system. With respect to support, participants across practice settings highlighted ongoing disruptions with system updates and the need to optimize within the EHR (e.g., templated notes, order sets) or rely on external support (e.g., medical scribes, dictation/transcription) to overcome challenges and maintain clinical productivity. Yet, those in smaller, private practices expressed added concern about the cost and overhead of these services.
Discussion
The near-universal adoption of EHRs in the United States has led to widespread changes in the practice of medicine. While this has been described broadly, surgeons have a specialized clinical workflow that combines patient care and procedures across multiple settings that may affect how the EHR can be leveraged to improve surgical quality. In this mixed methods study, we found that urologic surgeons use a multitude of EHR functions and feel that the EHR improves patient care. However, the negative impact on clinical efficiency continues to be an ongoing challenge and primarily relates to information management and administrative burden. This study also uncovers an emerging digital divide based on years in practice and lower versus higher-resourced settings that could limit the implementation and scalability of EHR-based tools.
While some negative sentiment persists, these data underscore the ubiquitous nature of EHR systems and growing acceptance. In the 2014 National EHR Survey, 78% of surgical specialists had adopted an EHR and 47% used all basic functions (i.e., prescription order entry, record clinical notes/medications/allergies/problem lists, and view laboratory results). 28 That same year, in another national survey of physicians, 23% agreed that the EHR improved efficiency and 62.5% disagreed (net favorability −39.5%), while 36.3% agreed that the EHR improved patient care and 41.0% disagreed (net favorability −4.7%). 29 Although specialty-specific responses to these questions were not reported, those in urology and other surgical specialties reported similar overall satisfaction with the EHR and less satisfaction with the clerical burden relative to the entire cohort. 29 Five years later, our findings indicate substantive progress with urologic surgeons reporting near universal use of EHR and its core functions, less negative attitudes with respect to clinical efficiency, and net positive perceptions on patient care. Moreover, newer entrants into the urologic workforce (i.e., ≤10 years in practice) have even better ratings for clinical efficiency (+7.5%) and patient care (+29.9%), likely due to the significant EHR exposure in contemporary training. 30 In summation, these findings suggest growing acceptance of the EHR, which may continue with subsequent generations of surgeons.
While encouraging, our findings also highlight ongoing challenges with the EHR that surgeons feel hamper clinical efficiency and patient care. Similar to other specialties, these center on information management and administrative burden. 31 Although the EHR provides greater access to information, surgeons often find it to be excessive, unstructured, and disorganized, increasing their work burden to sort and process it, interfering with patient interactions, and potentially leading to patient harms. 32 Additionally, surgeons expressed dissatisfaction with frequent, nonclinical tasks in the EHR that take significant time to complete. 31 Prior time-motion studies involving orthopedic and head and neck surgeons showed that physicians spend one-third of their in-room time with patients on EHR tasks while an EHR log study found that academic surgeons spend 14 h/wk in the EHR. 20 21 22 Although less than primary care and medical physicians, surgeons may be particularly pressed due to time spent in the operating room. 19 Notably, 35% of total EHR time for surgeons take place in remote and after-hour settings compared to 26 to 31% for nonsurgeons. 19 21 These demands, in turn, can interfere with the interpersonal dynamic between patients and physicians. 33 While prior studies mostly in the medical setting suggest a negligible impact on patient satisfaction, changes in face-to-face encounters in surgery have been shown to hamper communication, perceived empathy, and potentially trust, which are instrumental in avoiding adverse events and subsequent dissatisfaction and litigation. 32 34 35 When considered along with the feeling of not “practicing at top of license,” it should be unsurprising that the EHR has been found to be a major driver of burnout and dissatisfaction in the urologic and surgical workforces. 36 37
Finally, our study highlights differences across practice settings that may affect how surgeons use the EHR and their embrace of EHR-based tools. In this study, urologic surgeons in private practice used fewer EHR functions and had more negative perceptions of the EHR compared to colleagues in academic practices or large, integrated health systems. These findings may represent carryover from the slower uptake of the EHR by solo providers and physician-owned practices and may now be manifesting as less optimal utilization and lower user satisfaction. 8 15 28 38 At the same time, private practice surgeons report more burnout and less career satisfaction than counterparts in academics due in part to the EHR. 39 While this difference is likely multifactorial, private practice surgeons typically see more patients and take more call and may not have residents or advanced practice providers to share in the workload. 21 Similarly, resource constraints, especially among smaller practices, may limit access to medical scribes, new dictation technology, redesigned staffing models, and other staff support that improve productivity and provider satisfaction with the EHR. 40 41 So while broader trends are encouraging, a divide with respect to the EHR appears to be emerging between higher and lower-resourced practices.
These findings should be considered in the context of several limitations. First, there is potential for nonresponse bias. To address this concern, the AUA administers the survey through mixed modes and provides sampling weights to generate national estimates. Additionally, the 2,081 survey responses rank among the highest for surgeons in this topic area, while the 21% response rate compares favorably to similar studies. 9 16 29 36 Second, nonresponse bias could trickle down to the qualitative interviews. For this reason, we purposefully sampled based on years in practice, workload, and attitudes to ensure diverse views, and our cohort appears reflective of the overall workforce as indicated in Table 1 . Third, though this study examines a single surgical specialty, our cohort captures those practicing office-based urology, endourology, female pelvic floor and reconstruction, pediatric urology, and urologic oncology that have similarities to other surgical specialties. Furthermore, whereas medical specialties varied greatly in their EHR adoption, surgical specialties clustered closer together, suggesting some degree of homogeneity. 9 15 16 17 18 Fourth, interviews occurred during the coronavirus disease 2019 (COVID-19) pandemic, which could have altered the experiences and feelings elicited about the EHR. To the extent possible, the trained qualitative interviewers redirected conversations toward the interviewees' broader experience with the EHR as opposed to COVID-specific issues. Finally, based on the study design, we do not quantify the relative importance of themes identified in the qualitative interviews. On balance, this should be considered along with the strengths of the mixed methods study design that enable greater contextualization and insight into the survey findings.
These limitations notwithstanding, our findings have important implications for health IT in urology and potentially surgery more broadly. Increasingly, surgeons have looked to the EHR as a quality lever. This includes recent efforts to develop automated performance measurement, risk prediction, and clinical decision support among other interventions. 42 43 While promising, these EHR-based tools have been primarily developed and tested in the academic setting. Nearly half of urologists and surgeons, however, provide care in the private practice setting, which have both different experiences and resources. 36 37 Given this divide, it may be prudent to specifically engage the community and private practice surgeons in design to optimize workflows and ensure usability. 31 In fact, when engaged, surgeons in private practice can be quick adopters relative to counterparts in larger institutional settings. As an example, an electronic national quality registry in urology that extracts information automatically from EHRs has seen much greater uptake among private practice urologists as the initiative also addressed a specific need of private groups to meet quality reporting requirements. 44 In taking such an approach and in combination with broader efforts to improve the usability of the EHR, new EHR-based tools may see accelerated success, scaled across the surgical landscape.
Conclusion
Even with near universal adoption, urologic surgeons harbor mixed feelings for the EHR, particularly those in practice longer and in smaller, less resourced settings. Based on these findings, EHR-based tools designed to facilitate information management and minimize administrative burden, promote patient safety and the patient-surgeon relationship, and engage surgeons from varied settings, may be best positioned for effective use and provider satisfaction in the future.
Clinical Relevance Statement
While the use and perceptions of EHRs have improved, multiple challenges remain, particularly information management and administrative burden. Among surgeons, these dissatisfiers appear to be amplified by the procedure-based nature of the specialty, especially for those with less EHR exposure, infrastructure, and support. Efforts to transform surgical care delivery through the EHR will need to engage these surgeons specifically to find scalable success.
Multiple-Choice Questions
-
Which EHR function is used by only a minority of practicing urologic surgeons?
Chart review
Order entry
Pop-up/alerts
Secure messaging
Correct Answer : The correct answer is option c. In 2019, 43.4% of survey respondents reported that they routinely use information from pop-up or alerts such as BPAs.
-
Which characteristic is significantly associated with differences in EHR perceptions?
Subspecialty
Fellowship
Practice type
Minutes per visit
Correct Answer : The correct answer is option c. In the multivariable analysis, practice type was significantly associated with EHR use and positive perception for impact on clinical efficiency and patient care.
Funding Statement
Funding H.-J. T., MD, MSHPM was supported by a Mentored Research Scholar Grant in Applied and Clinical Research, MRSG-18-193-01-CPPB, from the American Cancer Society as well as the NIH Loan Repayment Program. The national survey was conducted through the American Urological Association (AUA) with approval and support from the AUA Data Committee and the AUA Data Management and Statistical Analysis team. The qualitative interviews were conducted through UNC CHAI Core, which receives funding support from National Cancer Institute grant P30-CA16086 to the UNC Lineberger Comprehensive Cancer Center.
Conflict of Interest None declared.
Protection of Human and Animal Subjects
The study was performed in compliance with the World Medical Association Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects. It was reviewed by UNC Institutional Review Board. The study did not involve any animal subjects.
References
- 1.McDermott K W.(IBM Watson Health), Freeman WJ (AHRQ), Elixhauser A (AHRQ). Overview of Operating Room Procedures During Inpatient Stays in U.S. Hospitals, 2014. HCUP Statistical Brief #233. December 2017. Agency for Healthcare Research and Quality. Rockville, MD. Accessed August 9, 2022 at:https://www.hcup-us.ahrq.gov/reports/statbriefs/sb233-Operating-Room-Procedures-United-States-2014.pdf [PubMed]
- 2.McDermott K W.(IBM Watson Health), Liang L (AHRQ). Overview of Major Ambulatory Surgeries Performed in Hospital-Owned Facilities, 2019. HCUP Statistical Brief #287. December 2021. Agency for Healthcare Research and Quality. Rockville, MD. Accessed August 9, 2022 at:https://www.hcup-us.ahrq.gov/reports/statbriefs/sb287-Ambulatory-Surgery-Overview-2019.pdf [PubMed]
- 3.Bongiovanni T, Parzynski C, Ranasinghe I, Steinman M A, Ross J S.Unplanned hospital visits after ambulatory surgical caremedRxiv 2021;2021.2003.2010.21249910 [DOI] [PMC free article] [PubMed]
- 4.Brown C S, Montgomery J R, Neiman P U. Assessment of potentially preventable hospital readmissions after major surgery and association with public vs private health insurance and comorbidities. JAMA Netw Open. 2021;4(04):e215503. doi: 10.1001/jamanetworkopen.2021.5503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kaye D R, Luckenbaugh A N, Oerline M. Understanding the costs associated with surgical care delivery in the Medicare population. Ann Surg. 2020;271(01):23–28. doi: 10.1097/SLA.0000000000003165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.American Recovery and Reinvestment Act of 2009. In: Congress US, edu. P.L. 111–52009
- 7.Non-federal Acute Care Hospital Electronic Health Record Adoption Health IT Quick-Stat #47. Office of the National Coordinator for Health Information Technology. Accessed August 9, 2022 at:https://www.healthit.gov/data/quickstats/non-federal-acute-care-hospital-electronic-health-record-adoption
- 8.Office-based Physician Electronic Health Record Adoption Health IT Quick-Stat #50. Office of the National Coordinator for Health Information Technology. Accessed August 9, 2022 at:https://www.healthit.gov/data/quickstats/office-based-physician-electronic-health-record-adoption
- 9.Myrick K L, Ogburn D F.Percentage of office-based physicians using any electronic health record (EHR)/electronic medical record (EMR) system and physicians that have a certified EHR/EMR system, by specialty: National Electronic Health Records Survey, 2017. January 2019. National Center for Health Statistics, Centers for Disease Prevention and Control. Accessed August 9, 2022 at:https://www.cdc.gov/nchs/data/nehrs/2017_NEHRS_Web_Table_EHR_Specialty.pdf
- 10.Parasrampuria S, Henry J.Hospitals' Use of Electronic Health Records Data, 2015–2017. ONC Data Brief, no.46. April 2019. Office of the National Coordinator for Health Information Technology. Washington, DC. Accessed August 9, 2022 at:https://www.healthit.gov/sites/default/files/page/2019-04/AHAEHRUseDataBrief.pdf
- 11.HITEC Investigators . Kaushal R, Edwards A, Kern L M, Investigators H. Association between electronic health records and health care utilization. Appl Clin Inform. 2015;6(01):42–55. doi: 10.4338/ACI-2014-10-RA-0089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lammers E J, McLaughlin C G, Barna M. Physician EHR adoption and potentially preventable hospital admissions among Medicare beneficiaries: panel data evidence, 2010-2013. Health Serv Res. 2016;51(06):2056–2075. doi: 10.1111/1475-6773.12586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Das M, Eichner J.Challenges and Barriers to Clinical Decision Support (CDS) Design and Implementation Experienced in the Agency for Healthcare Research and Quality CDS Demonstrations. 2010. Agency for Healthcare Research and Quality. Rockville, MD [Google Scholar]
- 14.with the HITEC Investigators . Ancker J S, Edwards A, Nosal S, Hauser D, Mauer E, Kaushal R. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med Inform Decis Mak. 2017;17(01):36. doi: 10.1186/s12911-017-0430-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kokkonen E W, Davis S A, Lin H C, Dabade T S, Feldman S R, Fleischer A B., JrUse of electronic medical records differs by specialty and office settings J Am Med Inform Assoc 201320(e1):e33–e38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Grinspan Z M, Banerjee S, Kaushal R, Kern L M. Physician specialty and variations in adoption of electronic health records. Appl Clin Inform. 2013;4(02):225–240. doi: 10.4338/ACI-2013-02-RA-0015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Yang N, Hung E.Table of Electronic Health Record Adoption and Use among Office-based Physicians in the U.S., by Specialty: 2015 National Electronic Health Records Survey. 2017. National Center for Health Statistics, Centers for Disease Control and Prevention. Accessed August 9, 2022 at:https://www.cdc.gov/nchs/data/ahcd/nehrs/2015_nehrs_ehr_by_specialty.pdf
- 18.Scanlon P.Evaluation of the 2015 National Electronic Health Records Survey. 2016. National Center for Health Statistics, Centers for Disease Control and Prevention. Accessed August 9, 2022 at:https://wwwn.cdc.gov/qbank/report/Scanlon_2016_NCHS_NEHRS.pdf
- 19.Rotenstein L S, Holmgren A J, Downing N L, Bates D W. Differences in total and after-hours electronic health record time across ambulatory specialties. JAMA Intern Med. 2021;181(06):863–865. doi: 10.1001/jamainternmed.2021.0256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sinsky C, Colligan L, Li L. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. 2016;165(11):753–760. doi: 10.7326/M16-0961. [DOI] [PubMed] [Google Scholar]
- 21.Cox M L, Risoli T, Jr, Peskoe S B, Turner D A, Migaly J. Quantified electronic health record (EHR) use by academic surgeons. Surgery. 2021;169(06):1386–1392. doi: 10.1016/j.surg.2020.12.009. [DOI] [PubMed] [Google Scholar]
- 22.Ebbers T, Kool R B, Smeele L E, Takes R P, van den Broek G B, Dirven R. Quantifying the electronic health record burden in head and neck cancer care. Appl Clin Inform. 2022;13(04):857–864. doi: 10.1055/s-0042-1756422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Shenson J A, Cronin R M, Davis S E, Chen Q, Jackson G P. Rapid growth in surgeons' use of secure messaging in a patient portal. Surg Endosc. 2016;30(04):1432–1440. doi: 10.1007/s00464-015-4347-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Seu M, Cho B H, Pigott R. Trends and perceptions of electronic health record usage among plastic surgeons. Plast Reconstr Surg Glob Open. 2020;8(04):e2709. doi: 10.1097/GOX.0000000000002709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Frazee R, Harmon L, Papaconstantinou H T. Surgeons' perspective of a newly initiated electronic medical record. Proc Bayl Univ Med Cent. 2016;29(01):21–23. doi: 10.1080/08998280.2016.11929344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Creswell J, Plano Clark V. Thousand Oaks, CA: Sage Publications; 2017. Designing and Conducting Mixed Methods Research. [Google Scholar]
- 27.Hsieh H F, Shannon S E. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(09):1277–1288. doi: 10.1177/1049732305276687. [DOI] [PubMed] [Google Scholar]
- 28.Heisey-Grove D, Patel V.Any, Certified, or Basic: Quantifying Physician EHR AdoptionONC Data Brief, no. 28. September 2015.Washington, DC: Office of the National Coordinator for Health Information Technology
- 29.Shanafelt T D, Dyrbye L N, Sinsky C. Relationship between clerical burden and characteristics of the electronic environment with physician burnout and professional satisfaction. Mayo Clin Proc. 2016;91(07):836–848. doi: 10.1016/j.mayocp.2016.05.007. [DOI] [PubMed] [Google Scholar]
- 30.Holmgren A J, Lindeman B, Ford E W. Resident physician experience and duration of electronic health record use. Appl Clin Inform. 2021;12(04):721–728. doi: 10.1055/s-0041-1732403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Dymek C, Kim B, Melton G B, Payne T H, Singh H, Hsiao C J. Building the evidence-base to reduce electronic health record-related clinician burden. J Am Med Inform Assoc. 2021;28(05):1057–1061. doi: 10.1093/jamia/ocaa238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Nijor S, Rallis G, Lad N, Gokcen E. Patient safety issues from information overload in electronic medical records. J Patient Saf. 2022;18(06):e999–e1003. doi: 10.1097/PTS.0000000000001002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Alkureishi M A, Lee W W, Lyons M. Impact of electronic medical record use on the patient-doctor relationship and communication: a systematic review. J Gen Intern Med. 2016;31(05):548–560. doi: 10.1007/s11606-015-3582-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kratzke I M, Rosenbaum M E, Cox C, Ollila D W, Kapadia M R. Effect of clear vs standard covered masks on communication with patients during surgical clinic encounters: a randomized clinical trial. JAMA Surg. 2021;156(04):372–378. doi: 10.1001/jamasurg.2021.0836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Boothman R C, Imhoff S J, Campbell D A., Jr Nurturing a culture of patient safety and achieving lower malpractice risk through disclosure: lessons learned and future directions. Front Health Serv Manage. 2012;28(03):13–28. [PubMed] [Google Scholar]
- 36.Mahoney S T, Strassle P D, Schroen A T.Survey of the US surgeon workforce: practice characteristics, job satisfaction, and reasons for leaving surgery J Am Coll Surg 202023003283–293..e1 [DOI] [PubMed] [Google Scholar]
- 37.The State of Urology Workforce and Practice in the United States 2021. 2022. American Urological Association. Linthicum, MD. Accessed August 9, 2022 at:https://www.AUAnet.org/common/pdf/research/census/State-Urology-Workforce-Practice-US.pdf
- 38.Jamoom E W, Heisey-Grove D, Yang N, Scanlon P. Physician opinions about EHR use by EHR experience and by whether the practice had optimized its EHR use. J Health Med Inform. 2016;7(04):1.00024E6. doi: 10.4172/2157-7420.1000240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Mahoney S T, Irish W, Strassle P D. Practice characteristics and job satisfaction of private practice and academic surgeons. JAMA Surg. 2021;156(03):247–254. doi: 10.1001/jamasurg.2020.5670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.McCormick B J, Deal A, Borawski K M. Implementation of medical scribes in an academic urology practice: an analysis of productivity, revenue, and satisfaction. World J Urol. 2018;36(10):1691–1697. doi: 10.1007/s00345-018-2293-8. [DOI] [PubMed] [Google Scholar]
- 41.Rotenstein L S, Apathy N, Landon B, Bates D W. Assessment of satisfaction with the electronic health record among physicians in physician-owned vs non-physician-owned practices. JAMA Netw Open. 2022;5(04):e228301. doi: 10.1001/jamanetworkopen.2022.8301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ren Y, Loftus T J, Datta S. Performance of a machine learning algorithm using electronic health record data to predict postoperative complications and report on a mobile platform. JAMA Netw Open. 2022;5(05):e2211973. doi: 10.1001/jamanetworkopen.2022.11973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Loftus T J, Tighe P J, Filiberto A C. Artificial intelligence and surgical decision-making. JAMA Surg. 2020;155(02):148–158. doi: 10.1001/jamasurg.2019.4917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Shelton J B, Pichardo D, Meeks W. Characteristics of participants in the American Urological Association Quality (AQUA) Registry and early impact of participation on quality of care. Urol Pract. 2021;8(02):209–216. doi: 10.1097/UPJ.0000000000000198. [DOI] [PubMed] [Google Scholar]