Download
1 / 30
360 likes | 583 Views
Respiratory viruses. Dr. Maeve M. Doyle SpR in Clinical Microbiology. Respiratory Viruses. Influenza Parainfluenzaviruses Respiratory syncitial virus (RSV) Rhinovirus Adenovirus Coronavirus – SARS Human metapneumovirus. Clinical syndromes. Bronchiolitis RSV Parainfluenzavirus

E N D
Respiratory viruses Dr. Maeve M. Doyle SpR in Clinical Microbiology
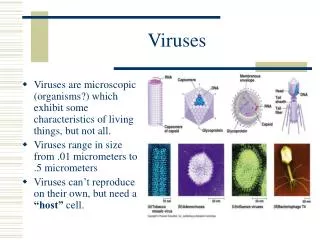
Respiratory Viruses • Influenza • Parainfluenzaviruses • Respiratory syncitial virus (RSV) • Rhinovirus • Adenovirus • Coronavirus – SARS • Human metapneumovirus
Clinical syndromes • Bronchiolitis • RSV • Parainfluenzavirus • Adenovirus • Croup • RSV • Parainfluenzavirus • Influenzavirus • Measles virus
Clinical syndromes cont’d • Upper respiratory tract • Rhinovirus • Coronavirus • Adenovirus • Influenzavirus • Parainfluenzavirus • RSV • Enterovirus • Influenza • Influenza A and B • Tonsillitis • EBV • Adenovirus
Clinical syndromes cont’d • Pneumonia • Influenza • Adenovirus • RSV • Parainfluenza • Enterovirus • CMV • VZV • Infectious mononucleosis • EBV • CMV
Respiratory Syncitial Virus • LRTI in young children • Bronchiolitis • Usually children under 12 months • Wheezing, increased respiratory rate. Cyanosis and apnoea in severe. • Pneumonia • May be life threatening • URTI in adults • Common cold • Elderly may develop pneumonia
Respiratory Syncitial Virus • The Virus • RNA virus • Family Paramyxoviridae • Therapy • Ribavirin • Given as an aerosol • Reduces virus shedding and duration of illness • Laboratory diagnosis • Detect antigen by immunofluoresence or ELISA • Culture
Rhinovirus • Most frequent cause of common cold (approx half) • Droplet spread • Incubation period 2-4 days • Limited to URT • The virus • RNA virus • Family Picornaviridae • >100 different serotypes • Therapy • Not available • Laboratory diagnosis • Culture
Coronovirus • Second most common cause of common cold (15-20%) • Usually milder infection • 50% of infection may be asymptomatic • Exception is SARS CoV • The virus • RNA virus • Family Coronaviridae • Club shaped spikes on surface (crown-like on EM)
Adenovirus • Infections of respiratory tract, the eye, the GIT. • Transmission by droplet and contact • Incubation period 5-10 days • Usually causes URTI • 50% of infections are asymptomatic • Occaisionally severe bronchopneumonia in infants • May cause whooping cough-like disease. • The virus • DNA virus • 47 or more serotypes • Therapy – not available • Laboratory diagnosis • Viral antigen detection by IF,ELISA and PCR • Culture • CF antibody titre – paired sera
Human metapneumovirus • Discovered in 2001 • Related to RSV • Infection in infants and young children • May be mild URTI • Bronchiolitis • Pneumonia • Therapy – none available
Parainfluenzavirus • Major cause of croup, bronchiolitis and pneumonia. • Second to RSV as cause of serious RTI in infants and children • Four serotypes • Transmission is by contact or droplet spread. • The virus • RNA virus • Family Paramyxoviridae • Therapy – none available • Laboratory diagnosis • Culture, PCR, antigen detection by IF • Serodiagnosis by paired sera 1-3 weeks apart
Influenza • Sixth leading cause of death in Canada • Responsible for between7000 and 72000 deaths in the US in any given year. • Studies have shown, that between 4-39% of adults hospitalised with CAP have evidence of viral infection • UK study, Thorax 2001: • 267 patients with CAP • 23% had evidence of viral infection • 20% with influenza (4% with RSV)
Influenzavirus • Causes illness in all age groups • Transmitted by aerosols • Mean incubation period is 2 days (1-4) • Symptoms • Sudden onset • Fever, chills, myalgia • Complications include secondary bacterial pneumonia, rarely viral pneumonia, myocarditis, encephalitis. Reyes syndrome has been associated with influenza B • Laboratory diagnosis • IF • EM • Serology • Culture
Influenza - the virus • RNA virus (orthomyxovirus group) • Large virus • Confined to infecting cells of URT and LRT • Viraemia is rarely detected • Three types A,B,C • B and C are believed to have man as the only host • Type A is found in swine, birds, horses and man. • Two major proteins on the surface • Haemaglutinin (HA) • Neuraminidase(NA) • Segmented viral genome • Allows for formation of viral reassortants (recombinants) between different strains and subtypes.
The virus • Classified as A,B or C, based on antigenic differences in their nucleprotein(NP) and matrix (M1)protein. • Further subtyping is based on the antigenicity of the two surface glycoproteins H and N
Influenza - the virus • Two spikes on the viral envelope (surface antigen) • Haemagglutinin (H) • 15 subtypes • (viral attachment to cells) • Neuraminidase (N) • 9 subtypes • (viral release from infected cells) • In mammalian flu, those which have circulated widely are limited to three HA (H1,H2,H3) and two NA (N1,N2) • The surface antigens have a tendancy for antigenic variation. • A doubly infected host can give rise to a new virus Note: pathogenic avian flu viruses are generally of the H5 or H7 subtype.
Flu – Shift/Drift • Influenza would cease to exist except it has evolved ways of defeating the immune system. i.e. antigenic variation • DRIFT • This is due to a point mutation • Small changes affecting H and N – occur constantly • SHIFT • This is due to genetic reassortment, usually between species. • Only in influenza A • Major change in H or N • Sets the stage for a new pandemic
The History of Flu • H1N1 1918 to 1919 Spanish flu (related to swine virus) • H2N2 1957 Asian flu (reassortant between human and avian) • H3N2 1968 Hong Kong flu (reassortment) • H1N1 1977 Russian flu • H5N1 1997 Hong Kong (all genes avian) • H9N2 1999 Hong Kong (avian) • H5N1 2004 Vietnam(13) and Thialand(4) (avian)
Pathogenesis • H allows attachment of virus to respiratory epithelial cells via receptors. • Virus is transported into cytoplasm in an endosome. • Acid pH in the endosome activates/opens an ion channel called M2 Protein, allowing H+ ions to enter the virus. • The acidification of the virus is necessary for viral uncoating, an essential step in replication. NOTE: Flu B doesn’t have an M2 protein • N digests neuraminic acid in respiratory mucus, perhaps facilitating viral spread.
Anti-virals active against Flu • Two main classes of drug: • Ion channel blocker • Amantadine • Rimantidine • Neuramidase inhibitor • Zanamivir • Oseltamivir
Ion Channel Blockers • Disable M2 protein • Blocks viral internalisation • Prevent viral uncoating • The virus is rendered inert
Side effects • 0-15% incidence of ‘jitteriness’ • Insomnia • Nightmares • Rarely hallucinations
Neuramidase inhibitors • NAI drugs bind the active site on viral NA • Viral particles cannot exit cells easily • Tend to clump and not disperse, reducing their ability to infect other cells and attenuating the patients infection. NOTE: NAI’s are active against flu A and B.
Side effects of NAI • 8-10% incidence of nausea, vomiting lasts 1-2 days and is not severe • ??Zanamivir associated with worsening of asthma
Which anti-viral is best • No published trials have compared the two agent head to head. • Side effect of amantadine are a potential limitation to its use- nausea, dizziness, insomnia and amphetamine-like effects • Current treatment course is 5 days • Reduce dose in impaired renal function and elderly. • Development of resistant virus with amantadine. • Mutation in M2 protein • Inhaled zanamivir may be associated with bronchospasm. • NAI resistant isolates have been described but are uncommon
Flu vaccine • Egg grown virus (purified,formalin-inactivated and extracted with ether) • Reassortment of two strains, one a high-yielding lab-adapted strain, the other containing the required H and N • Influenza A (H3N2, H1N1 strains) and Influenza B • Strains reviewed annually • Protection in up to 70% • Contraindicated if egg protein allergy
H5N1 • 1961 First isolated from birds • 2003/2004 affected poultry in eight countries in Asia • >100 million birds died or were killed • 1997 first case of spread to a human in Hong Kong 6/18 died • Aug 2004 human cases in Vietnam and Thialand • Aug 2004-Oct2005 117 cases, 60 fatal • Human to human spread is rare • Mortality 50% of infected
SARS Co-V • First cases, Guangdong provence, China, 2002 • WHO issued global health alert March 2003 • July 2003, WHO declared the outbreak over. • Clinical picture • Fever >38C • Respiratory symptoms, SOB • CXR, with pneumonia • To diagnose, also needed history of exposure
SARS Co-V • Droplet and contact spread • Coronavirus • Laboratory diagnosis • Cell culture • PCR • Serology • EM