












Cholecystitis cholelithiasis-presentation
- 1. BILIARY TRACT DISORDER Ms. Anshu M.Sc Nursing KGMU Institute of Nursing
- 2. INTRODUCTION- Disorders of gallbladder and ducts are extremely common. Its more commonly affect people of sedentary life style and obesity.
- 3. EPIDEMIOLOGY In the united states alone, it is estimated that 20 million people have gall stones with approximately 1 million new cases developing each year. The most common conditions are gall stones and associated cholecystitis.
- 4. About 98% of clients who present with symptomatic gall bladder disease have gall stones. Malignancies and congenital anomalies are very rare.
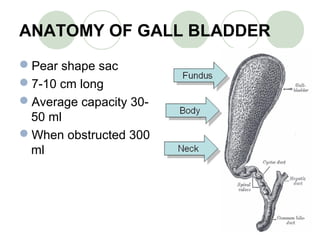
- 5. ANATOMY OF GALL BLADDER Pear shape sac 7-10 cm long Average capacity 30- 50 ml When obstructed 300 ml
- 6. PHYSIOLOGY OF GALL BLADDER The smooth muscles in the gallbladder wall contract, leading to the bile being secreted into the duodenum to rid the body of waste stored in the bile as well as aid in the absorption of dietary fat by solubilising them using bile acids.
- 7. BILE COMPOSITION Bile consists of water, electrolytes, bile acids, cholesterol, phospholipids and conjugated bilirubin Bile is secreted by the liver into small ducts that join to form the common hepatic duct and get stored in gall bladder.
- 8. BILIARY TRACT DISORDERS INCLUDES- Cholelithiasis Acute cholecystitis Chronic cholecystitis
- 9. CHOLELITHIASIS/ GALLSTONES Gallstones are collections of cholesterol, bile pigment or a combination of the two, which can form in the gallbladder or within the bile ducts of the liver.
- 10. Gallstones . . The presence of gallstones in the gallbladder is called cholelithiasis.
- 11. INCIDENCE Common duct stones are found in about 10% tom15% of client with cholelithiasis. The incidence increases with age, and the frequency of gallstones it the common duct in the older population may be as high as 25%.
- 12. ETIOLOGY Change in bile composition- Gallbladder stasis supersaturation of bile with cholesterol Infection and tissue injury Genetics
- 13. Those who are most at risk. These are all adjectives to describe the person most at risk of developing symptomatic gallstones. FAIR FAT FORTY FEMALE
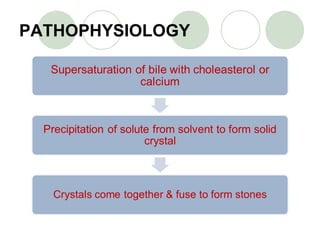
- 14. PATHOPHYSIOLOGY
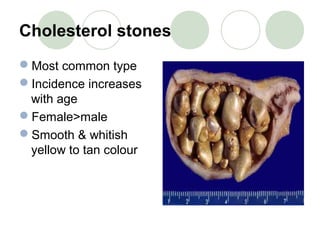
- 17. Cholesterol stones Most common type Incidence increases with age Female>male Smooth & whitish yellow to tan colour
- 18. Pigment stones Excess of unconjugated bilirubin May be black colour(associated with hemolysis and cirrhosis) or earthy calcium bilirubinate (associated with infection)
- 19. Mixed stones Combination of cholesterol and pigment stones or other substance Calcium carbonate,phosphate, bile salts, and palmitate
- 20. SIGNS AND SYMPTOMS. Complaints of indigestion after eating high fat foods. Localized pain in the right-upper quadrant epigastric region. Anorexia, nausea, vomiting and flatulence.
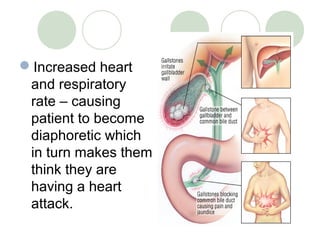
- 21. Increased heart and respiratory rate – causing patient to become diaphoretic which in turn makes them think they are having a heart attack.
- 22. SIGNS AND SYMPTOMS. Low grade fever. Elevated leukocyte count. Mild jaundice. Stools that contain fat – steatorrhea. Clay colored stools caused by a lack of bile in the intestinal tract. Urine may be dark amber- to tea-colored.
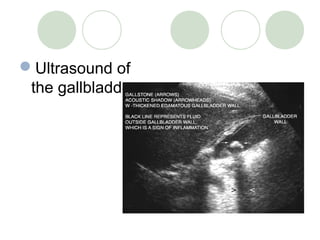
- 23. DIAGNOSTICS TEST History of patient Physical examination Laboratory test for- Elevated conjugated bilirubin. Elevated alkaline phosphate Serum amylase and lipase Elevated WBC count Fecal studies.
- 25. CT Scan MRI HIDA (hepato- iminodiacetic acid) Cholangiography ERCP (endoscopic retrograde cholangiopancreatography)
- 26. Diagnostics. HIDA (hydroxyiminod iacetic acid scan) - imaging test used to examine the gallbladder and the ducts leading into and out of the gallbladder - also referred to as cholescintigraphy.
- 27. MEDICAL MANAGEMENT GOALS- To resolve symptoms To remove stones To prevent complications
- 28. 1. PAIN MANAGEMENT Give analgesics Antacids, H2 blockers or proton pump inhibitors- to neutralize gastric acid 2.For nausea and vomiting Antiemetics given 3. antibiotics
- 29. Endoscopy
- 30. Gall stone dissolution Oral administration of agents- chenodeoxycholic acid (CDCA) or chenodal ursodeoxycholic acid (UDCA) or ursodiol Action- reduces the amount of cholesterol in bile
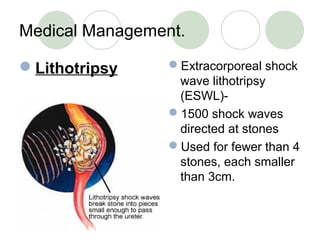
- 31. Medical Management. Lithotripsy Extracorporeal shock wave lithotripsy (ESWL)- 1500 shock waves directed at stones Used for fewer than 4 stones, each smaller than 3cm.
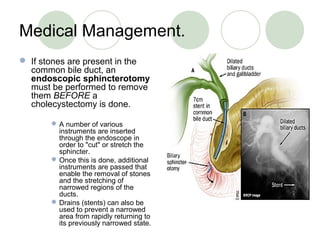
- 32. Medical Management. If stones are present in the common bile duct, an endoscopic sphincterotomy must be performed to remove them BEFORE a cholecystectomy is done. A number of various instruments are inserted through the endoscope in order to "cut" or stretch the sphincter. Once this is done, additional instruments are passed that enable the removal of stones and the stretching of narrowed regions of the ducts. Drains (stents) can also be used to prevent a narrowed area from rapidly returning to its previously narrowed state.
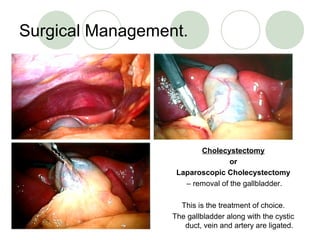
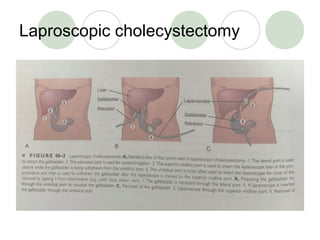
- 33. Surgical Management. Cholecystectomy or Laparoscopic Cholecystectomy – removal of the gallbladder. This is the treatment of choice. The gallbladder along with the cystic duct, vein and artery are ligated.
- 35. NURSING MANAGEMENT ASSESSMENT Assess the general condition of patient Assess pain of patient. Observe for bleeding.
- 36. NURSING DIAGNOSIS Acute pain related to surgical procedure. Impaired skin integrity Invasion of body structure Ineffective breathing pattern Pain Risk for deficient fluid volume related to surgical procedure
- 37. NURSING INTERVENTION 1. Acute pain related to surgery Monitor and record vital signs. administer medication as ordered. assess the severity,frequency, and characteristic of pain. Provide divertional activities such as reading newspapers.
- 38. 2. Impaired skin integrity Observe the color and character of the drainage. Change dressings as often as necessary. Place patient in low- or semi-Fowler’s position. Monitor puncture sites (3–5) if endoscopic procedure is done.
- 39. 3. Ineffective breathing pattern Observe respiratory rate, depth. Auscultate breath sounds. Assist patient to turn, cough, and deep breathe periodically. Show patient how to splint incision. Instruct in effective breathing techniques. Elevate head of bed, maintain low- Fowler’s position.
- 40. 4. Risk for deficient fluid volume Monitor vital signs. Assess mucous membranes, skin turgor, peripheral pulses, and capillary refill. Monitor I&O, including drainage from NG tube ,T-tube, and wound. Weigh patient periodically. Observe for signs of bleeding: hematemesis, melena, petechiae, ecchymosis. Administer IV fluids, blood products, as indicated
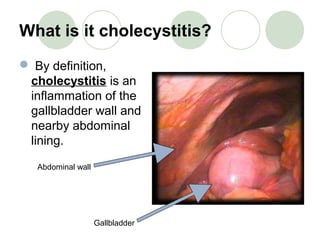
- 41. What is it cholecystitis? By definition, cholecystitis is an inflammation of the gallbladder wall and nearby abdominal lining. Abdominal wall Gallbladder
- 42. TYPES OF CHOLECYSTITIS Acute cholecystitis Chronic cholecystitis
- 43. ACUTE CHOLECYSTITIS DEFINITION- Acute cholecystitis refers to acute inflammation of the gallbladder wall.
- 44. ETIOLOGY Gall stone in cystic duct Obstruction in cystic duct Bacterial infection (gram positive and gram negative aerobes and anaerobes:- E. Coli, klebsiella, Clostredium and streptococcus)
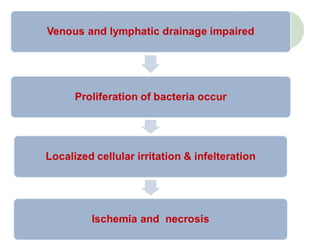
- 46. PATHOPHYSIOLOGY
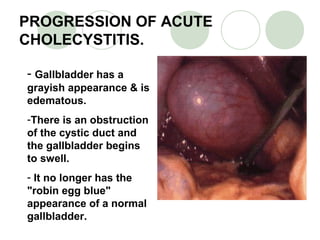
- 47. PROGRESSION OF ACUTE CHOLECYSTITIS. - Gallbladder has a grayish appearance & is edematous. -There is an obstruction of the cystic duct and the gallbladder begins to swell. - It no longer has the "robin egg blue" appearance of a normal gallbladder.
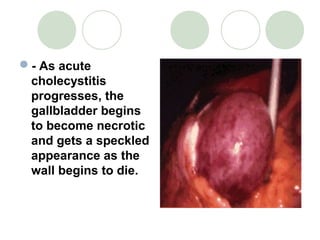
- 48. - As acute cholecystitis progresses, the gallbladder begins to become necrotic and gets a speckled appearance as the wall begins to die.
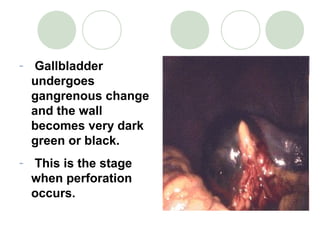
- 49. - Gallbladder undergoes gangrenous change and the wall becomes very dark green or black. - This is the stage when perforation occurs.
- 50. SIGNS AND SYMPTOMS Complain of pain In right upper quadrant In epigastric region In right subscapular Onset sudden Peak in 30min
- 51. Nausea and vomiting Low grade fever Mild jaundice
- 53. CHRONIC CHOLECYSTITIS DEFINITION- Repeated inflammation and infection of gallbladder
- 54. SIGNS AND SYMPTOMS Epigastric pain Indigestion Fat intolerance Heart burn Fibrosis of gall tissues Inability to concentrate bile
- 55. MEDICAL MANAGEMENT GOAL- to treat symptomatic causes to prevent complication
- 56. Antibiotic therapy- Ampicillin Ureidopenicillins – piperacillin or mezlocillin Third generation cephalosporins- Ceftriaxone, cefixime, Cefotaxime Aminoglycosides – Gentamicin, Amikacin, Neomycin
- 58. Nursing Interventions Post Op - Cholesystectomy 1. Administer oral analgesics to facilitate movement and deep breathing – and to stay ahead of pts pain. 2. Observe dressings frequently for exudate and hemorrhage. 3. Vitals are routinely checked. 4. Patient teaching: -Must understand how to splint the abd. before coughing. -Report any abnormalities such as, severe pain, tenderness in RUQ, increase in pulse, etc . . -Instructed that they usually can return to work in 3 days & can resume full activity in 1 week. 5. Fluid balance is maintained IV – potassium added to compensate for loss from surgery.
- 59. Nursing Interventions 1. Urine and stool should be observed for alterations in the presence of bilirubin. 2. NG tube must be monitored for amount, color & consistency of output. Also, tube must be on LOW suction and nasal area should be monitored for irritation and necrosis. 3. Anti-emetics may be administered if nausea persists. 4. I & O are measured and described carefully. 5. Pt. must understand how to splint the abdomen for post op coughing, turning and deep breathing. Interventions center on keeping patient comfortable by carefully administering meds and watching for reactions.
- 60. CONCLUSION Biliary disorders are extremely common but diverse in nature. Incidence rate of the disease is increasing day by day. Teaching and awareness is vital in prevention and management of the disease.
- 61. EVALUATION A 45 yr old obese lady, complaining of epigastric pain, right sided subscapular pain which last for 3-4 hrs associated with nausea and vomiting. She has mild icterus and bilirubin is 3.3mg/dl. Guess what could be the diagnosis of patient?