Superior vena cava syndrome
•Download as PPTX, PDF•
48 likes•8,061 views

This document discusses Superior vena cava syndrome (SVCS), which is caused by obstruction of the superior vena cava leading to symptoms like facial swelling and difficulty breathing. The document covers the history, anatomy, pathophysiology, clinical features, investigations, grading, and management of SVCS. It notes that while SVCS was once considered a medical emergency, it rarely causes immediate life-threatening issues now. Treatment depends on the underlying cause but may include supportive care, stents, chemotherapy, radiation therapy, or surgery. Radiation often provides symptom relief within 2 weeks for cancers like lung cancer.































































More Related Content
What's hot (20)
Similar to Superior vena cava syndrome (20)


















Recently uploaded (20)




















Superior vena cava syndrome
- 1. Superior vena cava syndrome DR AMIT P JOSE DEPARTMENT OF PULMONARY MEDICINE AIMS, KOCHI
- 2. HISTORY
- 3. HISTORY ▪ First recorded description of SVC obstruction (SVCO) - 1757 when William Hunter described the entity in a patient with a syphilitic aortic aneurysm. ▪ For nearly two centuries- nonmalignant processes such as aortic aneurysms, syphilitic aortitis, or chronic mediastinitis due to tuberculosis were the predominant etiologic factors. ▪ Now Rare
- 4. ▪ In the preantibiotic era- ▪ syphilitic thoracic aortic aneurysms, ▪ fibrosing mediastinitis, ▪ untreated infection were frequent causes of the SVC syndrome. ▪ Subsequently, malignancy became the most common cause, accounting for 90 percent of cases by the 1980s. ▪ More recently, the incidence of SVC syndrome due to thrombosis has risen, largely because of increased use of intravascular devices such as catheters and pacemakers. ▪ Benign causes now account for 20 to 40 percent of cases of SVC syndrome.
- 5. ▪ Once considered a medical emergency. ▪ SVCO rarely experience immediate, life-threatening complications.
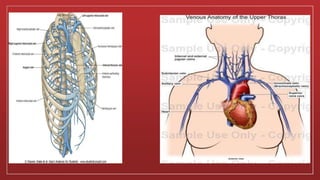
- 6. ANATOMY
- 9. ▪ Behind the lower border of the first right costal cartilage. ▪ Azygos vein joins it just before it enters the right atrium, at the upper right front portion of the heart. ▪ Distal 2 cm lying within the pericardial sac ▪ Formed by the joining of the internal jugular and subclavian veins. ▪ No valve divides the superior vena cava from the right atrium. ▪ As a result, the (right) atrial and (right) ventricular contractions are conducted up into the internal jugular vein and, through the sternocleidomastoid muscle, can be seen as the jugular venous pressure.
- 11. SVC SYNDROME ▪ Constellation of signs and symptoms caused by obstruction of blood flow in superior vena cava. ▪ External compression ▪ Invasion ▪ Constriction ▪ Thrombosis of SVC ▪ Partial or complete obstruction
- 12. Pathophysiology
- 13. Pathophysiology ▪ Right lung. ▪ Lymph nodes. ▪ Mediastinal structures. ▪ Thrombosis of blood within SVC.
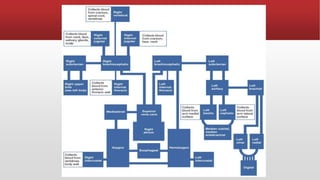
- 14. ▪ Collateral veins may arise from the azygos, internal mammary, lateral thoracic, paraspinous, and esophageal venous systems . ▪ The venous collaterals dilate over several weeks. ▪ Upper body venous pressure is markedly elevated initially but decreases over time. ▪ Symptoms and signs from SVC obstruction depends upon the rate at which complete obstruction of the SVC occurs in relation to the recruitment of venous collaterals.
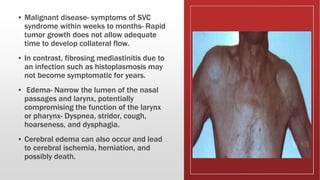
- 15. ▪ Malignant disease- symptoms of SVC syndrome within weeks to months- Rapid tumor growth does not allow adequate time to develop collateral flow. ▪ In contrast, fibrosing mediastinitis due to an infection such as histoplasmosis may not become symptomatic for years. ▪ Edema- Narrow the lumen of the nasal passages and larynx, potentially compromising the function of the larynx or pharynx- Dyspnea, stridor, cough, hoarseness, and dysphagia. ▪ Cerebral edema can also occur and lead to cerebral ischemia, herniation, and possibly death.
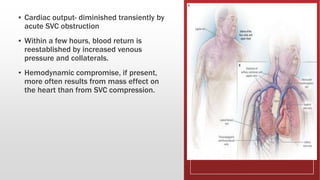
- 16. ▪ Cardiac output- diminished transiently by acute SVC obstruction ▪ Within a few hours, blood return is reestablished by increased venous pressure and collaterals. ▪ Hemodynamic compromise, if present, more often results from mass effect on the heart than from SVC compression.
- 17. Malignancy Fibrosing mediastinitis Pacemaker wires Post radiation fibrosis Central venous catheters
- 18. Clinical features of SVC Shortness of breath Chest pain Cough Dysphagia
- 19. Increased Venous pressure Edema of head, neck, arms and upper chest Dilated veins on chest wall Pleural/ pericardial effusion Cerebral edema/ increased IC pressure
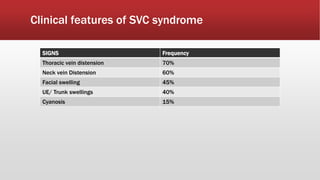
- 20. Clinical features of SVC syndrome SIGNS Frequency Thoracic vein distension 70% Neck vein Distension 60% Facial swelling 45% UE/ Trunk swellings 40% Cyanosis 15%
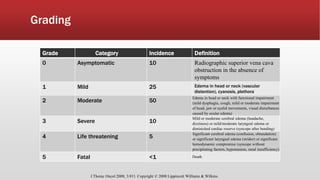
- 21. Grading Grade Category Incidence Definition 0 Asymptomatic 10 Radiographic superior vena cava obstruction in the absence of symptoms 1 Mild 25 Edema in head or neck (vascular distention), cyanosis, plethora 2 Moderate 50 Edema in head or neck with functional impairment (mild dysphagia, cough, mild or moderate impairment of head, jaw or eyelid movements, visual disturbances caused by ocular edema) 3 Severe 10 Mild or moderate cerebral edema (headache, dizziness) or mild/moderate laryngeal edema or diminished cardiac reserve (syncope after bending) 4 Life threatening 5 Significant cerebral edema (confusion, obtundation) or significant laryngeal edema (stridor) or significant hemodynamic compromise (syncope without precipitating factors, hypotension, renal insufficiency) 5 Fatal <1 Death J Thorac Oncol 2008; 3:811. Copyright © 2008 Lippincott Williams & Wilkins.
- 22. Why SVC ▪ Surrounded by rigid structures ▪ Thin walled easily Compressible ▪ Prone to obstruction
- 23. Consequence of SVCS ▪ Venous collaterals ▪ Severity of symptoms depends on time course of obstruction
- 24. Collaterals ▪ Thoracic venous collaterals: ▪ Azygos- hemiazygos- accessory hemiazygos system ▪ Vertebral and subscapular plexuses ▪ Mediastnal venous plexus and esophageal venous plexus and diaphragmatic venous plexus ▪ Lateral thoracic and superficial thoracoabdominal venous plexus ▪ Abominal venous collaterals
- 25. INVESTIGATION
- 26. Radiologic •CXR •CT •MRI •USG •Contrast enhanced venography •Tc 99m scan Histologic •Bone marrow biopsy •Lymph node biopsy •Sputum/ pleural fluid cytology •Bronchoscopy •Thoracentesis •Thoracotomy
- 27. Chest Radiograph ▪ Mediastinal widening. ▪ Venous collaterals:Large Azygous vein ▪ Mediastinal/ hilar mass ▪ Pleural effusion ▪ Calcifications
- 28. Contrast enhanced chest CT ▪ Defines the level and extent of venous blockage. ▪ Identification of the underlying cause of venous obstruction. ▪ Identify and map collateral pathways of venous drainage ▪ Presence of collateral vessels on CT is a strong indicator of SVC syndrome, Specificity of 96 percent and sensitivity of 92 percent. ▪ Contrast-enhanced blood from the collateral circulation draining into the inferior vena cava can simulate the appearance of a liver "hot spot" on CT
- 30. Venography ▪ Bilateral upper extremity venography is the gold standard for identification of SVC obstruction and the extent of associated thrombus formation. ▪ Superior to CT for defining the site and extent of SVC obstruction and for visualizing collateral pathways. ▪ It does not identify the cause of SVC obstruction unless thrombosis is the sole etiology. ▪ Radionuclide technetium-99m venography to assess SVC patency and venous flow patterns does not provide the important diagnostic information that is supplied by chest CT. ▪ Helical CT with bilateral upper extremity contrast injection (helical CT phlebography) appears to combine the diagnostic benefit of CT with the same degree of enhanced vascular detail as digital venography, as long as appropriate techniques for intravenous injection of contrast material are used to minimize flow artifacts arising from unopacified blood. ▪ Neither approach is warranted unless an intervention (placement of an endovascular stent, surgery) is planned.
- 32. MR venography ▪ Magnetic resonance venography (MRI) is an alternative approach that may be useful for patients with contrast dye allergy or those for whom venous access cannot be obtained for contrast enhanced studies
- 33. Ultrasonography ▪ Exclusion of thrombus in upper extremity, axillary, subclavian, and brachiocephalic veins.
- 34. Histologic diagnosis ▪ The clinical history combined with CT imaging will generally differentiate between benign causes of SVC obstruction (particularly caval thrombosis) and extrinsic compression related to malignancy. ▪ Histologic diagnosis is a prerequisite for choosing appropriate therapy for the patient with SVC syndrome associated with malignancy.
- 35. TREATMENT
- 36. Medical •Thrombolytics •Anticoagulants •Diuretics and corticosteroids Chemotherapy •NHL •Germ cell tumour •Limited stage small cell carcinoma Radiation •80-90 % relieved Surgical treatment •Bypass Endovascular treatment •Minimally invasive •Thrombolysis,angioplasty, stent placement
- 37. ▪ SVC syndrome associated with malignancy ▪ Alleviate symptoms and treat the underlying disease. ▪ The average life expectancy among patients who present with malignancy-associated SVC syndrome is approximately six months. ▪ But there is wide variability depending on the underlying malignancy. ▪ Treatment of SVC syndrome and its underlying cause results in long-term relapse-free survival and cure. ▪ Most likely to be achieved in chemotherapy-sensitive malignancies using a combined modality treatment approach. ▪ Evidence-based guidelines for management of SVC syndrome are not available. ▪ A general recommendation supporting radiotherapy or stent placement for symptomatic SVC syndrome from lung cancer has been made by both the National Comprehensive Cancer Network (NCCN) and the American College of Chest Physicians . ▪ Initial management should be guided by the severity of symptoms and the underlying malignant condition as well as the anticipated response to treatment.
- 38. Need for emergent RT ?????? ▪ Emergency RT is no longer considered necessary for most patients for several reasons: ▪ Symptomatic obstruction is often a prolonged process developing over a period of weeks or longer prior to clinical presentation. ▪ Deferring therapy until a full diagnostic work-up has been completed does not pose a hazard for most patients, provided the evaluation is efficient and the patient is clinically stable. ▪ illustrated in a review of 107 cases of SVC syndrome, in which no serious complication resulted from the SVC obstruction itself or investigative procedures leading to the diagnosis despite a prolonged period between the onset of symptoms and the initiation of therapy in some cases. ▪ RT prior to biopsy may obscure the histologic diagnosis. ▪ One study of 19 patients with symptomatic mediastinal masses who received emergency RT, a histologic diagnosis could not be established in eight (42 percent) from a biopsy obtained after such treatment. ▪ Current management guidelines-accurate histologic diagnosis prior to starting therapy and the upfront use of endovascular stents in severely symptomatic patients to provide more rapid relief than can be achieved using RT.
- 39. Exception ▪ Patients who present with stridor due to ▪ central airway obstruction ▪ severe laryngeal edema, and ▪ those with coma from cerebral edema. ▪ These situations represent a true medical emergency, and these patients require immediate treatment (stent placement and RT) to decrease the risk of sudden respiratory failure and death.
- 40. Supportive care and medical management ▪ No data documenting the effectiveness of this maneuver, the head should be raised to decrease hydrostatic pressure and head and neck edema. ▪ Obstruction of blood flow through the SVC slows venous return. This can result in local irritation or thrombosis of veins in the upper extremities, or delayed absorption of drugs from the surrounding tissues. Thus, the use of intramuscular injections in the arms should be avoided. ▪ For patients who have obstruction of the SVC resulting from intravascular thrombus associated with an indwelling catheter, removal of the catheter is indicated, in conjunction with systemic anticoagulation.
- 41. Glucocorticoids ▪ Two settings in which systemic administration of glucocorticoids may be helpful. ▪ Symptomatology due to SVC syndrome caused by steroid- responsive malignancies such as lymphoma or thymoma. ▪ In patients undergoing RT, particularly if laryngeal edema is present, glucocorticoids are commonly prescribed to reduce swelling. ▪ Only case reports to suggest benefit.
- 42. Diuretics ▪ Diuretics are also commonly recommended, although it is unclear whether venous pressures distal to the obstruction are affected by small changes in right atrial pressure. ▪ In a retrospective series of 107 patients with SVC syndrome from a variety of causes, the rate of clinical improvement was similar among patients receiving glucocorticoids, diuretics, or both
- 43. Chemotherapy for small cell lung cancer, NHL, and germ cell tumors ▪ Initial chemotherapy is the treatment of choice for patients with symptomatic SVC syndrome. ▪ Clinical response to chemotherapy alone is usually rapid. ▪ When chemotherapy is the initial intervention of choice and the SVC obstruction is unrelieved, chemotherapy should be administered through a dorsal foot vein . ▪ Symptomatic improvement usually occurs within one to two weeks of treatment initiation. In a review of treatment for SVC obstruction in patients with lung cancer, chemotherapy alone relieved symptoms of SVC obstruction in 77 percent of those with SCLC, although 17 percent had a later recurrence. ▪ For these malignancies, use of RT alone usually yields poorer long-term results and may compromise the subsequent results of chemotherapy . ▪ Certain situations (eg, limited stage SCLC, some subtypes of NHL), the addition of RT to systemic chemotherapy may decrease local recurrence rates and improve overall survival.
- 44. ▪ Among patients with SVC syndrome and NHL, symptoms suggesting involvement of other mediastinal structures (eg, dysphagia, hoarseness or stridor) and shorter symptom duration appear to be adverse prognostic factors
- 45. Non-small cell lung cancer ▪ As compared with more therapy-sensitive malignancies, the degree and rapidity of response to chemotherapy is less in NSCLC. ▪ Symptom relief in this setting is more rapidly achieved by the use of an endovascular stent. ▪ SVC obstruction is a strong predictor of poor prognosis in patients with NSCLC, with a median survival of only five months in one series. ▪ Long-term relapse-free survival has been rarely reported in patients with locally advanced disease and SVC syndrome treated with chemotherapy alone or a combined modality approach that includes both RT and chemotherapy, therapy of SVC syndrome in patients with NSCLC is most often directed toward palliation of symptoms rather than long-term remission. For previously unirradiated patients, palliation is most often achieved with external beam irradiation.
- 46. Radiation therapy ▪ Radiation therapy (RT) is widely advocated for SVC syndrome caused by radiosensitive tumors in patients who have not been previously irradiated. ▪ Most of the malignancies causing SVC syndrome are radiation-sensitive, and at least in lung cancer, symptomatic improvement is usually apparent within 72 hours. ▪ In a systematic review, RT was associated with complete relief of symptoms of SVC obstruction within two weeks in 78 and 63 percent of patients with SCLC and NSCLC, respectively.The rates of relapse post-treatment were 17 and 19 percent for SCLC and NSCLC, respectively. ▪ Objective measurement of the change in vena caval obstruction may not parallel measures of symptomatic improvement. ▪ In an autopsy series,complete and partial SVC patency was found in only 14 and 10 percent of patients after RT for SVC syndrome, despite reported relief of symptoms in 85 percent. These data have led some to suggest that the development of collateralization may have contributed more to symptomatic improvement than the effect of RT, and to question the value of urgent RT in patients with SVC syndrome from chemotherapy sensitive malignancies. ▪ Relief of symptoms may not be achieved for up to four weeks, and approximately 20 percent of patients do not obtain symptomatic relief from RT. F ▪ urthermore, the benefits of RT are often temporary, with many patients developing recurrent symptoms before dying of the underlying disease. ▪ Particularly if symptoms are severe, more rapid palliation can be achieved through the use of an intraluminal stent, followed by RT for disease control. Stent placement is also effective in relieving symptoms in patients who fail to respond to RT.
- 47. Endovascular Stents ▪ Indications: ▪ Stent can be placed before a tissue diagnosis is available ▪ Useful procedure for patients with severe symptoms who require urgent intervention. ▪ An endovascular stent is particularly appropriate for rapid symptom palliation in patients with NSCLC and mesothelioma and for those with recurrent disease who have previously received systemic therapy or RT. ▪ The role of endovascular stenting in patients presenting with chemotherapy sensitive tumors (ie, SCLC, NHL, germ cell tumors) and SVC obstruction is uncertain.
- 48. ▪ Self-expanding endovascular stent restores venous return and provides rapid and sustained symptom palliation in patients with SVC syndrome. ▪ The technical success rate is in the range of 95 to 100 percent, and over 90 percent of patients report relief of symptoms. ▪ The stent is placed percutaneously via the internal jugular, subclavian, or femoral vein, under local anesthetic. A guide wire is manipulated through the stenosis or obstruction in order to deploy the metal stent across the lesion. One stent may not be sufficient to bridge the entire extent of the stenotic area, particularly with involvement of the brachiocephalic veins. Sometimes two or even three stents in series ("kissing stents"). ▪ Total occlusion of the SVC is not necessarily a contraindication to intraluminal stent placement nor is the presence of thrombus within a stenotic area. In such cases, balloon angioplasty or catheter-directed thrombolysis or mechanical thrombectomy could be considered prior to stent placement.
- 49. ▪ There appears to be no significant difference in the published outcomes of the three most commonly used stainless steel stents (Gianturco Z stent, the Palmaz stent, or the Wallstent) .There are newer self-expanding stents (Luminex, Smart, Protege) made from nitinol (a nickel-titanium alloy) that exhibit shape memory effect and superelasticity. They have some advantages over the first- generation stents including a greater precision in placement within a stenotic area, lower thrombogenicity, and a higher radial force that allows them to withstand extrinsic compression and better maintain long-term patency. Covered stents may have higher long- term patency rates as compared to uncovered stents, but additional experience is needed.
- 50. ▪ Systematic review of the literature of patients with SVC obstruction due to lung cancer (either SCLC or NSCLC) . ▪ 159 patients who underwent stent placement, 95 percent had relief of symptoms, and the incidence of reocclusion (usually due to thrombosis or tumor ingrowth into the stent) was only 11 percent. ▪ In contrast, of the over 600 patients with SCLC, chemotherapy alone, chemoradiotherapy, and RT resulted in complete or partial relief of symptoms in 84, 94, and 78 percent of cases, respectively. ▪ Among 150 patients with NSCLC, approximately 60 percent had relief with chemotherapy or RT. Overall, relapse rates were lower with SVC stenting (11 versus 17 to 19 percent with RT and/or chemotherapy) in both SCLC and NSCLC.
- 51. Thrombolytic therapy ▪ When extensive thrombosis occurs as a complication of SVC stenosis, local catheter-directed thrombolytic therapy may be of value to reduce the length of the obstruction and the number and length of stents required, and also reduce the risk of embolization. ▪ The thrombus may also be removed by mechanical thrombectomy, although this is used less often than thrombolysis. ▪ Thrombolytic therapy has also been administered following placement of an endovascular stent in an attempt to decrease secondary reocclusion. ▪ Benefit of thrombolytics- unclear, and increase the risk of hematoma, gastrointestinal hemorrhage, hemoptysis and epistaxis. ▪ In a systematic review, the morbidity of stent insertion was greatest when thrombolytics were also administered, and there was no evidence that reocclusion rates were lower . Thus, this approach is not generally recommended.
- 52. Need for long-term anticoagulation ??????? ▪ Short-term anticoagulation is often recommended after stent placement but whether long-term anticoagulation is necessary is an area of uncertainty. ▪ To prevent stent reocclusion, some advocate anticoagulation for periods of one to nine months while others suggest antiplatelet therapy alone. ▪ There are no data upon which to form an evidence-based recommendation: warfarin 1 mg daily with the goal of maintaining an INR of less than 1.6 is a reasonable approach. ▪ An alternative approach is dual antiplatelet therapy (eg, clopidogrel 75 mg daily plus aspirin) for three months after stent placement.
- 53. Complications of stent placement ▪ 3 to 7 percent of patients. ▪ Early complications include infection, pulmonary embolus, stent migration, hematoma at the insertion site, bleeding, and rarely, perforation or rupture of the SVC. ▪ Late complications include bleeding (1 to 14 percent) and death (1 to 2 percent) from anticoagulation and stent failure with reocclusion. ▪ Stent failure is most often caused by thrombus or tumor ingrowth. ▪ Most patients with malignancy-related SVC syndrome have a short life expectancy, the stent usually remains patent until death. ▪ If reocclusion does occur, it can be treated with a second stent or thrombolytic therapy, with good secondary patency rates.
- 54. Surgical intervention ▪ Surgical bypass is rarely performed in patients with malignant cause of SVC syndrome because of the success of endovascular stenting. ▪ Surgical management is more often undertaken in patients with benign causes of SVC syndrome. ▪ One possible exception is malignant thymoma and thymic carcinoma, which are relatively resistant to chemotherapy and radiation.
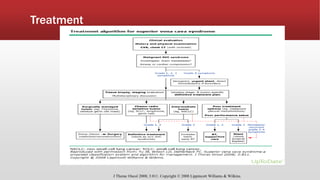
- 56. Treatment J Thorac Oncol 2008; 3:811. Copyright © 2008 Lippincott Williams & Wilkins.
- 57. Summary ▪ SVC syndrome results from extrinsic and intrinsic compression of SVC ▪ Clinical presentation depends on acuity of obstruction and adequate collateral development. ▪ Majority of svc due to malignancy ▪ Histologic diagnosis to guide treatment and determine prognosis.