25. basics of mechanical ventilation in neonates
•Download as PPT, PDF•
47 likes•6,068 views

This document provides an overview of mechanical ventilation in neonates. It discusses indications for mechanical ventilation, initial ventilator settings, monitoring the infant, weaning from ventilation, complications, and adjusting settings based on blood gas results. The goal is to optimize gas exchange while using the lowest possible oxygen and ventilator pressures. Settings are adjusted as needed based on the infant's condition and blood gas levels.
25. basics of mechanical ventilation in neonates
- 1. NNC Module: Basics of Mechanical Ventilation in Neonates Learning Objectives Slide 1 Learning ObjectivesLearning Objectives (cont.)(cont.) 7. Apply initial ventilator settings. 8. Adjust ventilator settings to improve oxygenation and ventilation as indicated 9. Monitor the neonate during mechanical ventilation. 10. Detect any deterioration during mechanical ventilation and identify its causes.
- 2. NNC Module: Basics of Mechanical Ventilation in Neonates Learning Objectives Slide 2 Learning ObjectivesLearning Objectives (cont.)(cont.) 11. Apply paralysis and sedation as needed. 12. Recognize how to wean the neonate from assisted ventilation. 13. Apply physiotherapy and suction to the neonate as indicated. 14. Detect complications that may occur during mechanical ventilation.
- 3. NNC Module: Basics of Mechanical Ventilation in Neonates Introduction Slide 3 IntroductionIntroduction Mechanical ventilation is an invasive life- support procedure with many effects on the cardiopulmonary system. The goal is to optimize both gas exchange and clinical status at minimum FiO2 and ventilator pressure. The ventilator strategy employed to accomplish this goal depends in part on the infant disease process.
- 4. NNC Module: Basics of Mechanical Ventilation in Neonates Indications of Mechanical Ventilation Slide 4 Indications of MechanicalIndications of Mechanical VentilationVentilation Absolute indicationsAbsolute indications If any of the following is present:If any of the following is present: 1. Severe hypoxemia with PaO2 less than 50 mmHg despite FiO2 of 0.8. 2. Respiratory acidosis with pH of less than 7.20 to 7.25, or PaCO2 above 60 mmHg. 3. Severe prolonged apnea.
- 5. NNC Module: Basics of Mechanical Ventilation in Neonates Indications of Mechanical Ventilation Slide 5 Indications of MechanicalIndications of Mechanical VentilationVentilation (cont.)(cont.) Relative indicationsRelative indications 1. Frequent intermittent apnea unresponsive to drug therapy. 2. Early treatment when use of mechanical ventilation is anticipated because of deteriorating gas exchange. 3. Relieving work of breathing in an infant with signs of respiratory difficulty. 4. Initiation of exogenous surfactant therapy in infants with RDS.
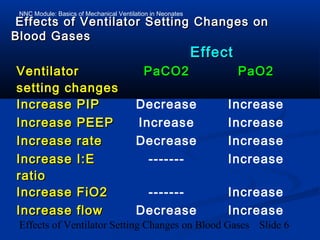
- 6. NNC Module: Basics of Mechanical Ventilation in Neonates Effects of Ventilator Setting Changes on Blood Gases Slide 6 Effects of Ventilator Setting Changes onEffects of Ventilator Setting Changes on Blood GasesBlood Gases EffectEffect VentilatorVentilator setting changessetting changes PaCO2PaCO2 PaO2PaO2 Increase PIPIncrease PIP Decrease Increase Increase PEEPIncrease PEEP Increase Increase Increase rateIncrease rate Decrease Increase Increase I:EIncrease I:E ratioratio ------- Increase Increase FiO2Increase FiO2 ------- Increase Increase flowIncrease flow Decrease Increase
- 7. NNC Module: Basics of Mechanical Ventilation in Neonates Starting Ventilator Setting Slide 7 Starting Ventilator SettingStarting Ventilator Setting Intubate infant with an endotracheal tube according to body weight. During intubation, infants require fractional inspired oxygen FiO2 that is 10% higher than what they were receiving before mechanical ventilation.
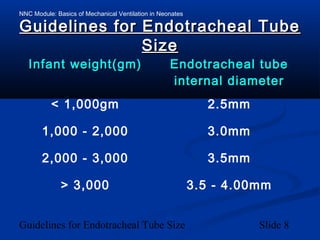
- 8. NNC Module: Basics of Mechanical Ventilation in Neonates Guidelines for Endotracheal Tube Size Slide 8 Guidelines for Endotracheal TubeGuidelines for Endotracheal Tube SizeSize Infant weight(gm)Infant weight(gm) Endotracheal tubeEndotracheal tube internal diameterinternal diameter < 1,000gm 2.5mm 1,000 - 2,000 3.0mm 2,000 - 3,000 3.5mm > 3,000 3.5 - 4.00mm
- 9. NNC Module: Basics of Mechanical Ventilation in Neonates Initial Setting of Mechanical Ventilation Slide 9 Initial Setting of MechanicalInitial Setting of Mechanical VentilationVentilation PIP is determined by hearing good breath sounds and good lung expansion. FiO2 is determined according to patient need. Ti should not be prolonged because of risk of alveolar over-distention. Start with 0.25 seconds and do not exceed 0.5 seconds (unless there are special indications). Respirator rate should not ordinarily exceed 80 breaths/min to allow sufficient time for exhalation.
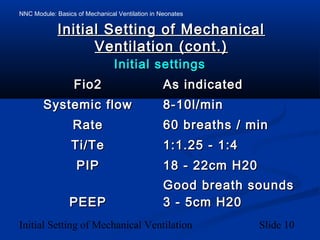
- 10. NNC Module: Basics of Mechanical Ventilation in Neonates Initial Setting of Mechanical Ventilation Slide 10 Initial Setting of MechanicalInitial Setting of Mechanical Ventilation (cont.)Ventilation (cont.) Initial settingsInitial settings Fio2Fio2 As indicatedAs indicated Systemic flowSystemic flow 8-10l/min8-10l/min RateRate 60 breaths / min60 breaths / min Ti/TeTi/Te 1:1.25 - 1:41:1.25 - 1:4 PIPPIP 18 - 22cm H2018 - 22cm H20 Good breath soundsGood breath sounds PEEPPEEP 3 - 5cm H203 - 5cm H20
- 11. NNC Module: Basics of Mechanical Ventilation in Neonates Subsequent Settings of Mechanical Ventilation Slide 11 Subsequent Settings ofSubsequent Settings of Mechanical VentilationMechanical Ventilation Measure arterial blood gases half an hour after the initial setting and adjust the setting accordingly. (Table) Although it is tempting to try to lower PaCO2 by increasing the respiratory rate rather than by adjusting ventilatory pressure, data suggest that this can not be without risk.
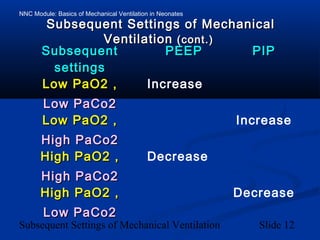
- 12. NNC Module: Basics of Mechanical Ventilation in Neonates Subsequent Settings of Mechanical Ventilation Slide 12 Subsequent Settings of MechanicalSubsequent Settings of Mechanical VentilationVentilation (cont.)(cont.) SubsequentSubsequent settingssettings PEEPPEEP PIPPIP Low PaO2 ,Low PaO2 , Low PaCo2Low PaCo2 Increase Low PaO2 ,Low PaO2 , High PaCo2High PaCo2 Increase High PaO2 ,High PaO2 , High PaCo2High PaCo2 Decrease High PaO2 ,High PaO2 , Low PaCo2Low PaCo2 Decrease
- 13. NNC Module: Basics of Mechanical Ventilation in Neonates Monitoring The Infant during Mechanical Ventilation Slide 13 Monitoring The Infant duringMonitoring The Infant during Mechanical VentilationMechanical Ventilation Obtain an initial blood gas within 15-30 minutes of starting mechanical ventilation. • Obtain a blood gas within 15-30 minutesObtain a blood gas within 15-30 minutes of any change in ventilator settings.of any change in ventilator settings. • Obtain a blood gas every 6 hours unlessObtain a blood gas every 6 hours unless a sudden change in the infant's conditiona sudden change in the infant's condition occurs.occurs. • Continuous monitoring of the O2Continuous monitoring of the O2 saturation level as well as the HR and RRsaturation level as well as the HR and RR is necessary.is necessary.
- 14. NNC Module: Basics of Mechanical Ventilation in Neonates Deterioration during Mechanical Ventilation Slide 14 Deterioration duringDeterioration during Mechanical VentilationMechanical Ventilation Sudden clinical deteriorationSudden clinical deterioration Mechanical or electrical ventilator failure. Disconnected tube or leaking connection. Endotracheal tube displacement or blockage. Pneumothorax.
- 15. NNC Module: Basics of Mechanical Ventilation in Neonates Deterioration during Mechanical Ventilation Slide 15 Deterioration duringDeterioration during Mechanical VentilationMechanical Ventilation (cont.)(cont.) Gradual deteriorationGradual deterioration Inappropriate ventilator setting. Intraventricular hemorrhage. Baby fighting against ventilator. PDA. Anemia. Infection.
- 16. NNC Module: Basics of Mechanical Ventilation in Neonates Paralysis and Sedation Slide 16 Paralysis and SedationParalysis and Sedation (cont.)(cont.) Sedation is useful when agitation interferes with ventilatory support and when infants fight the ventilator. Phenobarbital decreases the variability in mean arterial pressure and intracranial pressure associated with endotracheal suctioning.
- 17. NNC Module: Basics of Mechanical Ventilation in Neonates Weaning Slide 17 WeaningWeaning When the patient is stable, FiO2 and PIP are weaned first. Decrease PIP as tolerated and as chest rise diminishes. When PIP is around 20, attention is directed to FiO2 and then to the respiratory rate alternating with each other, in response to assessment of chest excursion, blood gas results, and oxygen saturation.
- 18. NNC Module: Basics of Mechanical Ventilation in Neonates Weaning Slide 18 WeaningWeaning (cont.)(cont.) As frequency is decreased, Te should be prolonged. For larger infants, weaning to endotracheal CPAP may begin when PIP has been stable between 15-18 cmH2O, and FiO2 is less than 0.4. The infant can be weaned to oxygen hood when he/she requires less than 4 cmH2O of end expiratory pressure.
- 19. NNC Module: Basics of Mechanical Ventilation in Neonates Weaning Slide 19 WeaningWeaning (cont.)(cont.) For infants weighing less than 1,750 gm, when PIP is less than 15 cmH2O and FiO2 is less than 0.3, start to decrease the respiratory rate gradually to 15-20 breaths/min and then wean directly to nasal CPAP if available. In most infants, when ventilator frequency of approximately 15 breaths per minute is tolerated, endotracheal CPAP may be tried for a short period before extubation.
- 20. NNC Module: Basics of Mechanical Ventilation in Neonates Weaning Slide 20 WeaningWeaning (cont.)(cont.) Atelectasis after extubation is common in preterm infants recovering from RDS. Use of nasal CPAP may prevent atelectasis. Steroids are not routine before extubation, but if there was prolonged intubation or previous failed attempts of extubation, a short course of steroids may facilitate extubation. If strider caused by laryngeal edema develops after extubation, racemic epinephrine aerosols and steroids may be helpful.
- 21. NNC Module: Basics of Mechanical Ventilation in Neonates Physiotherapy and Suctioning Slide 21 Physiotherapy andPhysiotherapy and SuctioningSuctioning Tracheal suctioning and chest physiotherapy should be minimized in infants with HMD in the first few days after birth because their secretions are scant. Physiotherapy and suctioning should be done to prevent the development of atelectasis, especially in premature infants. However, some infants show acute deterioration of blood gases.
- 22. NNC Module: Basics of Mechanical Ventilation in Neonates Complications of Mechanical Ventilation Slide 22 Complications of MechanicalComplications of Mechanical VentilationVentilation Endotracheal tube complications andEndotracheal tube complications and tracheal lesionstracheal lesions Accidental displacement of the endotracheal tube into main stem bronchus, hypopharynx, or esophagus. Accidental extubation. Obstruction of endotracheal tube.
- 23. NNC Module: Basics of Mechanical Ventilation in Neonates Complications of Mechanical Ventilation Slide 23 Complications of MechanicalComplications of Mechanical VentilationVentilation (cont.)(cont.) Airway injuryAirway injury Subglottic stenosis. Edema of the cords after extubation (may result in hoarseness and stridor). Prolonged use of orotracheal intubation associated with palatal groove formation. Necrotizing tracheobronchitis.
- 24. NNC Module: Basics of Mechanical Ventilation in Neonates Complications of Mechanical Ventilation Slide 24 Complications of MechanicalComplications of Mechanical VentilationVentilation (cont.)(cont.) InfectionInfection Pneumonia and systemic infections with Staphylococcus epidermidis, Candida organism, gram-negative organisms, and Staphylococcus aureus.
- 25. NNC Module: Basics of Mechanical Ventilation in Neonates Complications of Mechanical Ventilation Slide 25 Complications of MechanicalComplications of Mechanical VentilationVentilation (cont.)(cont.) Chronic lung disease / OxygenChronic lung disease / Oxygen toxicitytoxicity Bronchopulmonary dysplasia (BPD), related to increased airway pressure and changes in lung volume. Other contributing factors are oxygen toxicity, anatomic and physiologic immaturity, and individual susceptibility.
- 26. NNC Module: Basics of Mechanical Ventilation in Neonates Complications of Mechanical Ventilation Slide 26 Complications of MechanicalComplications of Mechanical VentilationVentilation (cont.)(cont.) Air leakAir leak Pneumothorax, pulmonary interstitial emphysema (PIE), and pneumomediastinum directly related to increased airway pressure occurring frequently at MAP >14 cmH2O.
- 27. NNC Module: Basics of Mechanical Ventilation in Neonates Complications of Mechanical Ventilation Slide 27 Complications of MechanicalComplications of Mechanical VentilationVentilation (cont.)(cont.) MiscellaneousMiscellaneous Intraventricular hemorrhage. Decreased cardiac output. Feeding intolerance