Anatomy of the Knee Joint
•
298 likes•128,525 views

The knee joint is a synovial joint between the femur, tibia, and patella that allows for flexion, extension, and some rotation, and contains cruciate ligaments, menisci, and surrounding muscles, nerves and blood vessels to support its complex movements and function as the body's largest joint.














Anatomy of the Knee Joint
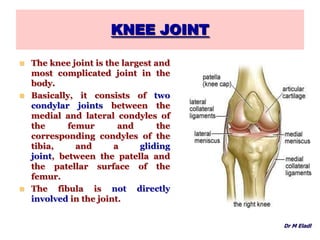
- 2. KNEE JOINT The knee joint is the largest and most complicated joint in the body. Basically, it consists of two condylar joints between the medial and lateral condyles of the femur and the corresponding condyles of the tibia, and a gliding joint, between the patella and the patellar surface of the femur. The fibula is not directly involved in the joint. Dr M Eladl
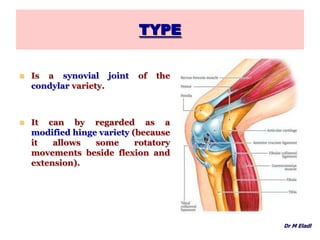
- 3. TYPE Is a synovial joint of the condylar variety. It can by regarded as a modified hinge variety (because it allows some rotatory movements beside flexion and extension). Dr M Eladl
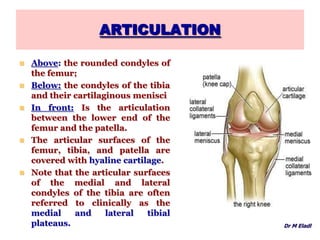
- 4. ARTICULATION Above: the rounded condyles of the femur; Below: the condyles of the tibia and their cartilaginous menisci In front: Is the articulation between the lower end of the femur and the patella. The articular surfaces of the femur, tibia, and patella are covered with hyaline cartilage. Note that the articular surfaces of the medial and lateral condyles of the tibia are often referred to clinically as the medial and lateral tibial plateaus. Dr M Eladl
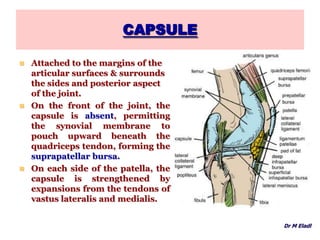
- 5. CAPSULE Attached to the margins of the articular surfaces & surrounds the sides and posterior aspect of the joint. On the front of the joint, the capsule is absent, permitting the synovial membrane to pouch upward beneath the quadriceps tendon, forming the suprapatellar bursa. On each side of the patella, the capsule is strengthened by expansions from the tendons of vastus lateralis and medialis. Dr M Eladl
- 6. CAPSULE Behind the joint, the capsule is strengthened by an expansion of the semimembranous muscle called the oblique popliteal ligament. An opening in the capsule behind the lateral tibial condyle permits the tendon of the popliteus to emerge. Dr M Eladl
- 7. LIGAMENTS Ligaments may be divided into 1) Extracapsular ligaments: Those that lie outside the capsule. 2) Capsular ligaments Those that are thickend parts of the capsule. 3) Intracapsular Ligaments Those that lie within the capsule. Dr M Eladl
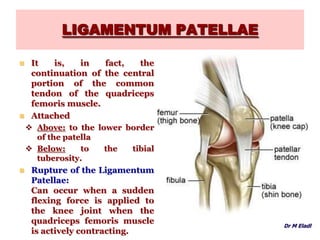
- 8. LIGAMENTUM PATELLAE It is, in fact, the continuation of the central portion of the common tendon of the quadriceps femoris muscle. Attached Above: to the lower border of the patella Below: to the tibial tuberosity. Rupture of the Ligamentum Patellae: Can occur when a sudden flexing force is applied to the knee joint when the quadriceps femoris muscle is actively contracting. Dr M Eladl
- 9. LATERAL COLLATERAL LIGAMENT Cordlike and is attached above to the lateral condyle of the femur and below to the head of the fibula. The tendon of popliteus muscle intervenes between the ligament and the lateral meniscus. Forced adduction of the tibia on the femur can result in injury to the lateral collateral ligament (less common than medial ligament injury). Dr M Eladl
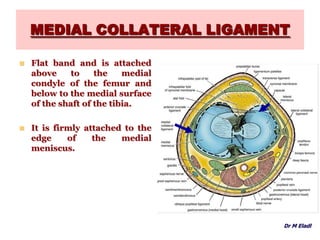
- 10. MEDIAL COLLATERAL LIGAMENT Flat band and is attached above to the medial condyle of the femur and below to the medial surface of the shaft of the tibia. It is firmly attached to the edge of the medial meniscus. Dr M Eladl
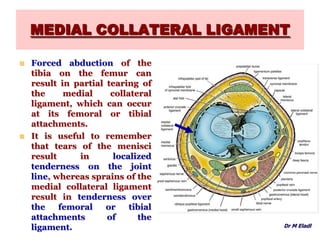
- 11. MEDIAL COLLATERAL LIGAMENT Forced abduction of the tibia on the femur can result in partial tearing of the medial collateral ligament, which can occur at its femoral or tibial attachments. It is useful to remember that tears of the menisci result in localized tenderness on the joint line, whereas sprains of the medial collateral ligament result in tenderness over the femoral or tibial attachments of the ligament. Dr M Eladl
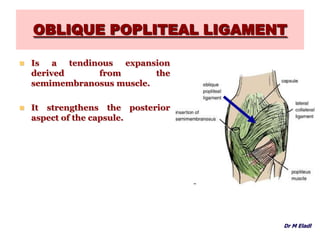
- 12. OBLIQUE POPLITEAL LIGAMENT Is a tendinous expansion derived from the semimembranosus muscle. It strengthens the posterior aspect of the capsule. Dr M Eladl
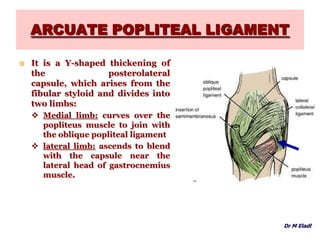
- 13. ARCUATE POPLITEAL LIGAMENT It is a Y-shaped thickening of the posterolateral capsule, which arises from the fibular styloid and divides into two limbs: Medial limb: curves over the popliteus muscle to join with the oblique popliteal ligament lateral limb: ascends to blend with the capsule near the lateral head of gastrocnemius muscle. Dr M Eladl
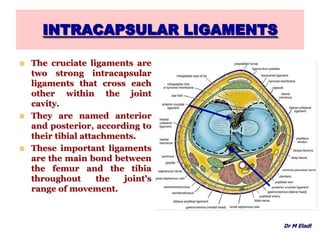
- 14. INTRACAPSULAR LIGAMENTS The cruciate ligaments are two strong intracapsular ligaments that cross each other within the joint cavity. They are named anterior and posterior, according to their tibial attachments. These important ligaments are the main bond between the femur and the tibia throughout the joint's range of movement. Dr M Eladl
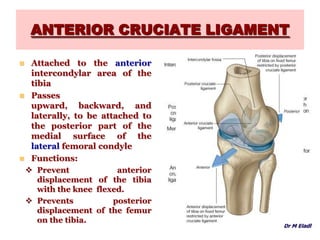
- 15. ANTERIOR CRUCIATE LIGAMENT Attached to the anterior intercondylar area of the tibia Passes upward, backward, and laterally, to be attached to the posterior part of the medial surface of the lateral femoral condyle Functions: Prevent anterior displacement of the tibia with the knee flexed. Prevents posterior displacement of the femur on the tibia. Dr M Eladl
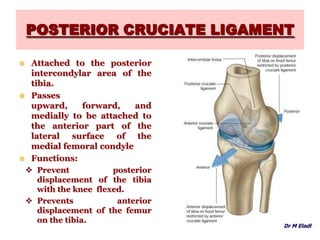
- 16. POSTERIOR CRUCIATE LIGAMENT Attached to the posterior intercondylar area of the tibia. Passes upward, forward, and medially to be attached to the anterior part of the lateral surface of the medial femoral condyle Dr M Eladl
- 17. POSTERIOR CRUCIATE LIGAMENT Attached to the posterior intercondylar area of the tibia. Passes upward, forward, and medially to be attached to the anterior part of the lateral surface of the medial femoral condyle Functions: Prevent posterior displacement of the tibia with the knee flexed. Prevents anterior displacement of the femur on the tibia. Dr M Eladl
- 18. MENISCI The menisci are C-shaped sheets of fibrocartilage. The upper surfaces are in contact with the femoral condyles. The lower surfaces are in contact with the tibial condyles. The peripheral border is thick and attached to the capsule The inner border is thin and concave and forms a free edge. Dr M Eladl
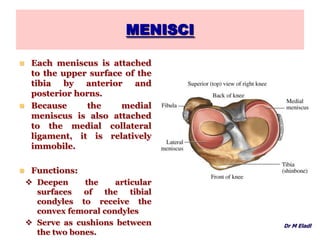
- 19. MENISCI Each meniscus is attached to the upper surface of the tibia by anterior and posterior horns. Because the medial meniscus is also attached to the medial collateral ligament, it is relatively immobile. Functions: Deepen the articular surfaces of the tibial condyles to receive the convex femoral condyles Serve as cushions between the two bones. Dr M Eladl
- 20. SYNOVIAL MEMBRANE Lines the capsule and is attached to the margins of the articular surfaces. On the front and above the joint, it forms a pouch, which extends up beneath the quadriceps femoris muscle for three fingerbreadths above the patella, forming the suprapatellar bursa. This is held in position by the attachment of a small portion of the vastus intermedius muscle, called the articularis genu muscle. Dr M Eladl
- 21. SYNOVIAL MEMBRANE At the back of the joint, it is prolonged on the deep surface of the tendon of the popliteus, forming the popliteal bursa. A bursa is interposed between the medial head of the gastrocnemius and the medial femoral condyle and the semimembranosus tendon; this is termed the semimembranosus bursa, and it frequently communicates with the synovial cavity of the joint. Dr M Eladl
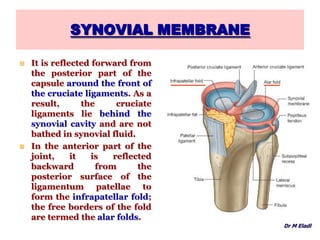
- 22. SYNOVIAL MEMBRANE It is reflected forward from the posterior part of the capsule around the front of the cruciate ligaments. As a result, the cruciate ligaments lie behind the synovial cavity and are not bathed in synovial fluid. In the anterior part of the joint, it is reflected backward from the posterior surface of the ligamentum patellae to form the infrapatellar fold; the free borders of the fold are termed the alar folds. Dr M Eladl
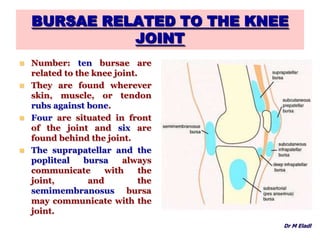
- 23. BURSAE RELATED TO THE KNEE JOINT Number: ten bursae are related to the knee joint. They are found wherever skin, muscle, or tendon rubs against bone. Four are situated in front of the joint and six are found behind the joint. The suprapatellar and the popliteal bursa always communicate with the joint, and the semimembranosus bursa may communicate with the joint. Dr M Eladl
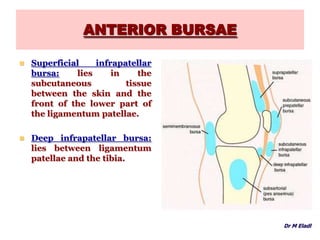
- 24. ANTERIOR BURSAE Suprapatellar bursa: lies beneath the quadriceps muscle and communicates with the joint cavity. Prepatellar bursa: lies in the subcutaneous tissue between the skin and the front of the lower half of the patella and the upper part of the ligamentum patellae. Dr M Eladl
- 25. ANTERIOR BURSAE Superficial infrapatellar bursa: lies in the subcutaneous tissue between the skin and the front of the lower part of the ligamentum patellae. Deep infrapatellar bursa: lies between ligamentum patellae and the tibia. Dr M Eladl
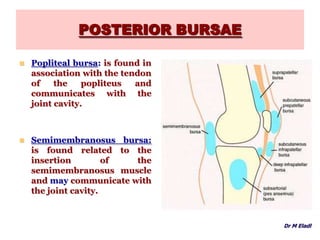
- 26. POSTERIOR BURSAE Popliteal bursa: is found in association with the tendon of the popliteus and communicates with the joint cavity. Semimembranosus bursa: is found related to the insertion of the semimembranosus muscle and may communicate with the joint cavity. Dr M Eladl
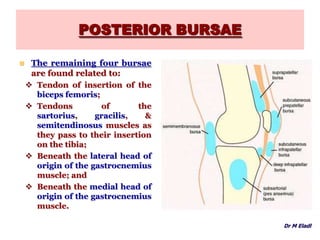
- 27. POSTERIOR BURSAE The remaining four bursae are found related to: Tendon of insertion of the biceps femoris; Tendons of the sartorius, gracilis, & semitendinosus muscles as they pass to their insertion on the tibia; Beneath the lateral head of origin of the gastrocnemius muscle; and Beneath the medial head of origin of the gastrocnemius muscle. Dr M Eladl
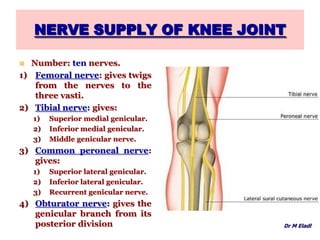
- 28. NERVE SUPPLY OF KNEE JOINT Number: ten nerves. 1) Femoral nerve: gives twigs from the nerves to the three vasti. 2) Tibial nerve: gives: 1) Superior medial genicular. 2) Inferior medial genicular. 3) Middle genicular nerve. 3) Common peroneal nerve: gives: 1) Superior lateral genicular. 2) Inferior lateral genicular. 3) Recurrent genicular nerve. 4) Obturator nerve: gives the genicular branch from its posterior division Dr M Eladl
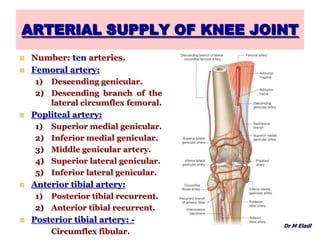
- 29. ARTERIAL SUPPLY OF KNEE JOINT Number: ten arteries. Femoral artery: 1) Descending genicular. 2) Descending branch of the lateral circumflex femoral. Popliteal artery: 1) Superior medial genicular. 2) Inferior medial genicular. 3) Middle genicular artery. 4) Superior lateral genicular. 5) Inferior lateral genicular. Anterior tibial artery: 1) Posterior tibial recurrent. 2) Anterior tibial recurrent. Posterior tibial artery: - Circumflex fibular. Dr M Eladl
- 30. MOVEMENT OF KNEE JOINT Flexion: Mainly by: biceps femoris, semitendinosus Assisted by: sartorius, gracilis and popliteus muscles. Extension: Mainly by: Quadriceps femoris muscle. Assisted by: tensor fasciae lata muscle. Medial rotation: Mainly by: popliteus muscle. Assisted by: sartorius, gracilis, semitendinosus & semimembranosus. Lateral rotation: Only done by the biceps femoris muscle. Dr M Eladl
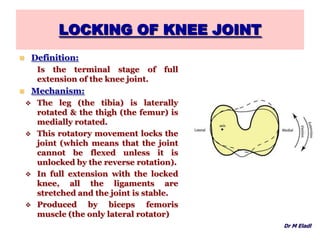
- 31. LOCKING OF KNEE JOINT Definition: Is the terminal stage of full extension of the knee joint. Mechanism: The leg (the tibia) is laterally rotated & the thigh (the femur) is medially rotated. This rotatory movement locks the joint (which means that the joint cannot be flexed unless it is unlocked by the reverse rotation). In full extension with the locked knee, all the ligaments are stretched and the joint is stable. Produced by biceps femoris muscle (the only lateral rotator) Dr M Eladl
- 32. UNLOCKING OF KNEE JOINT Dr M Eladl Definition: Is the early stage of flexion of the knee joint. Mechanism: The leg is medially rotated and the thigh is laterally rotated. Muscles produce unlocking: This is done by the action of: Popliteus muscle, helped by: Semimembranosus, semitendinos us & gracilis muscles
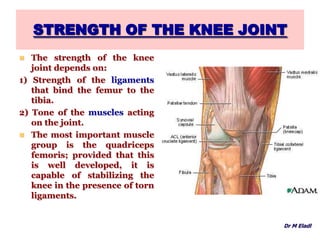
- 33. STRENGTH OF THE KNEE JOINT The strength of the knee joint depends on: 1) Strength of the ligaments that bind the femur to the tibia. 2) Tone of the muscles acting on the joint. The most important muscle group is the quadriceps femoris; provided that this is well developed, it is capable of stabilizing the knee in the presence of torn ligaments. Dr M Eladl
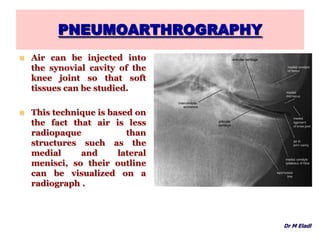
- 34. PNEUMOARTHROGRAPHY Air can be injected into the synovial cavity of the knee joint so that soft tissues can be studied. This technique is based on the fact that air is less radiopaque than structures such as the medial and lateral menisci, so their outline can be visualized on a radiograph . Dr M Eladl
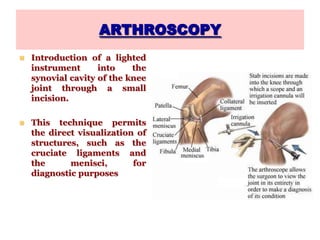
- 35. ARTHROSCOPY Introduction of a lighted instrument into the synovial cavity of the knee joint through a small incision. This technique permits the direct visualization of structures, such as the cruciate ligaments and the menisci, for diagnostic purposes
- 36. INJURIES OF THE KNEE JOINT Knee joint injuries are common because: 1. It is a low-placed joint. 2. Mobile. 3. Weight-bearing joint, 4. Serving as a fulcrum between two long levers (thigh and leg). 5. Its stability depends almost entirely on its associated ligaments and surrounding muscles. 6. The knee joint is essential for everyday activities such as standing, walking, and climbing stairs. 7. It is also a main joint for sports that involve running, jumping, kicking, and changing directions. To perform these activities, the knee joint must be mobile; however, this mobility makes it susceptible to injuries. Dr M Eladl
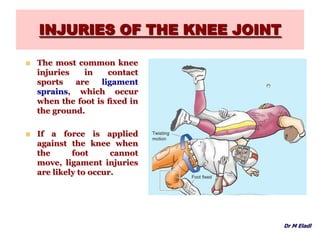
- 37. INJURIES OF THE KNEE JOINT The most common knee injuries in contact sports are ligament sprains, which occur when the foot is fixed in the ground. If a force is applied against the knee when the foot cannot move, ligament injuries are likely to occur. Dr M Eladl
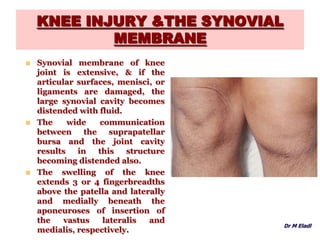
- 38. KNEE INJURY &THE SYNOVIAL MEMBRANE Synovial membrane of knee joint is extensive, & if the articular surfaces, menisci, or ligaments are damaged, the large synovial cavity becomes distended with fluid. The wide communication between the suprapatellar bursa and the joint cavity results in this structure becoming distended also. The swelling of the knee extends 3 or 4 fingerbreadths above the patella and laterally and medially beneath the aponeuroses of insertion of the vastus lateralis and medialis, respectively. Dr M Eladl
- 39. TIBIAL COLLATERAL LIGAMENT INJURY The firm attachment of the TCL to the medial meniscus is of considerable clinical significance because tearing of this ligament frequently results in concomitant tearing of the medial meniscus. This injury is common in athletes who twist their flexed knees while running (e.g. , in basketball, the various forms of football, and volleyball). Dr M Eladl
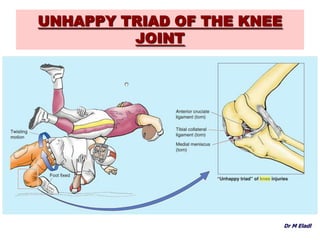
- 40. UNHAPPY TRIAD OF THE KNEE JOINT The ACL, which serves as a pivot for rotatory movements of the knee and is taut during flexion, may also tear subsequent to the rupture of the TCL, creating an “unhappy triad” of knee injuries. Dr M Eladl
- 41. UNHAPPY TRIAD OF THE KNEE JOINT Dr M Eladl
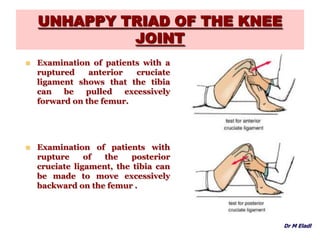
- 42. UNHAPPY TRIAD OF THE KNEE JOINT Examination of patients with a ruptured anterior cruciate ligament shows that the tibia can be pulled excessively forward on the femur. Examination of patients with rupture of the posterior cruciate ligament, the tibia can be made to move excessively backward on the femur . Dr M Eladl
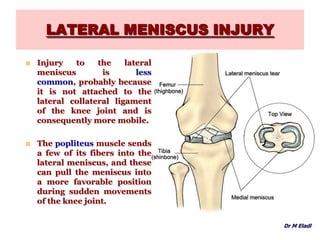
- 43. LATERAL MENISCUS INJURY Injury to the lateral meniscus is less common, probably because it is not attached to the lateral collateral ligament of the knee joint and is consequently more mobile. The popliteus muscle sends a few of its fibers into the lateral meniscus, and these can pull the meniscus into a more favorable position during sudden movements of the knee joint. Dr M Eladl
- 44. THANK YOU