C2 fracture
Download as PPTX, PDF1 like860 views

C2 fractures can range from asymptomatic to paralysis and are often caused by motor vehicle accidents or falls. Higher level cervical spine injuries carry greater risks. C2 fractures include odontoid fractures, lateral mass fractures, extension teardrop fractures, and traumatic spondylolisthesis (hangman's fracture). Diagnosis involves imaging like X-rays and CT/MRI to classify the fracture. Treatment depends on fracture type and severity but may include immobilization, traction, internal fixation, or fusion surgery. Complications can include malunion, nonunion, or pseudarthrosis if not properly treated.
































More Related Content
What's hot (20)
Similar to C2 fracture (20)


















Recently uploaded (20)




















C2 fracture
- 2. Background Cervical spine (C-spine) injuries are the most feared of all spinal injuries because of the potential for significant deleterious sequelae. Relation, higher the level of the C-spine injury higher the morbidity and mortality Craniocervical junction injuries are the deadliest.
- 3. MVA and fall are responsible for bulk of C2 fracture. The clinical manifestations range from asymptomatic to frank paralysis. Motor Vehicle Accident ER(unconscious patient) C-spine pathology (10%)
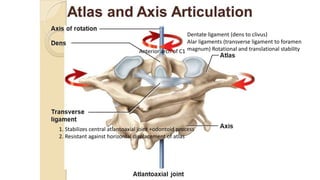
- 4. Anterior arch of C1 1. Stabilizes central atlantoaxial joint +odontoid process 2. Resistant against horizontal displacement of atlas Dentate ligament (dens to clivus) Alar ligaments (transverse ligament to foramen magnum) Rotational and translational stability
- 5. Pathogenesis
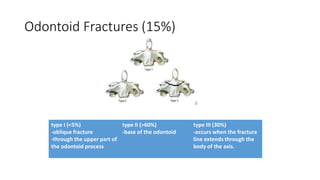
- 6. Odontoid Fractures (15%) type I (<5%) -oblique fracture -through the upper part of the odontoid process type II (>60%) -base of the odontoid type III (30%) -occurs when the fracture line extends through the body of the axis.
- 7. Mechanism: precise unknown, flexion, extension, rotation History: 1. Pain 2. Inability to actively move the neck 3. Sensation of instability (feeling of head being unstable on spine) 4. Holding head with hand to prevent motion Examination: Quadriplagia with respiratory system involvement to minimal upper- extremity motor and sensory deficit secondary to loss of one or more cervical nerve roots.
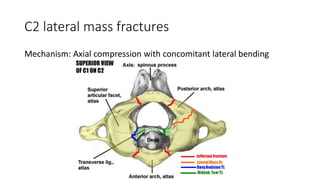
- 8. C2 lateral mass fractures Mechanism: Axial compression with concomitant lateral bending
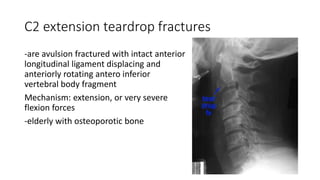
- 9. C2 extension teardrop fractures -are avulsion fractured with intact anterior longitudinal ligament displacing and anteriorly rotating antero inferior vertebral body fragment Mechanism: extension, or very severe flexion forces -elderly with osteoporotic bone
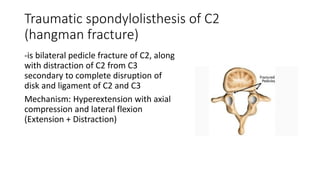
- 10. Traumatic spondylolisthesis of C2 (hangman fracture) -is bilateral pedicle fracture of C2, along with distraction of C2 from C3 secondary to complete disruption of disk and ligament of C2 and C3 Mechanism: Hyperextension with axial compression and lateral flexion (Extension + Distraction)
- 11. Physical Examination Motor • Sternocleidomastoid (SCM) • Trapezius Reflex SCM reflex, by tapping on clavicular end of muscle Sensory • Posterior scalp • Anterolateral neck • Antero inferior & postero inferior external ear
- 12. Clinical Examination • Observe and palpate deformities and step-offs • Test muscle strength and tone of upper and lower extremities • Perform sensory on upper and lower extremities • Perform rectal examination • Test trapezius muscles by asking patient to shrug shoulders • Observe for torticollis
- 13. Imaging Studies: AP/Lat/Odontoid views Xray C-spine (1st choice) CT C-spine (extent of injury) MRI (soft tissue injury, neural element injury and disk injury)
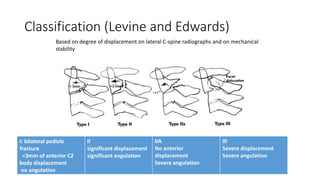
- 14. Classification (Levine and Edwards) Based on degree of displacement on lateral C-spine radiographs and on mechanical stability I: bilateral pedicle fracture <3mm of anterior C2 body displacement no angulation II significant displacement significant angulation IIA No anterior displacement Severe angulation III Severe displacement Severe angulation
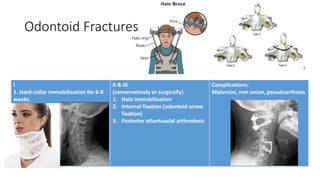
- 15. Odontoid Fractures I 1. Hard-collar immobilisation for 6-8 weeks II & III (conservatively or surgically) 1. Halo immobilisation 2. Internal fixation (odontoid screw fixation) 3. Posterior atlantoaxial arthrodesis Complications: Malunion, non union, pseudoarthosis
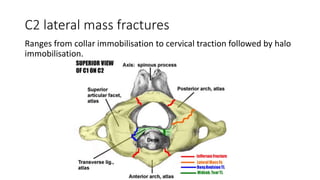
- 16. C2 lateral mass fractures Ranges from collar immobilisation to cervical traction followed by halo immobilisation.
- 17. C2 extension teardrop fractures Cervical orthosis
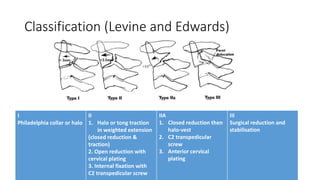
- 18. Classification (Levine and Edwards) I Philadelphia collar or halo II 1. Halo or tong traction in weighted extension (closed reduction & traction) 2. Open reduction with cervical plating 3. Internal fixation with C2 transpedicular screw IIA 1. Closed reduction then halo-vest 2. C2 transpedicular screw 3. Anterior cervical plating III Surgical reduction and stabilisation