Wound care
•
17 likes•20,119 views

This document provides an overview of wound care including wound healing processes, types of wounds, evaluation and documentation of wounds, and wound management. It discusses the stages of wound healing including hemostasis, inflammation, proliferation, and remodeling. Different types of wounds such as incisions, lacerations, abrasions, and puncture wounds are described along with factors to evaluate like location, size, exudate, signs of infection, and surrounding tissue condition. Methods of documentation including photography and standardized descriptions are covered. The management section addresses wound care plans, cleaning, debridement, exudate management using various dressing materials, and treatment of infections.


































Wound care
- 1. WOUND CARE 2016. 3. 10 STAFF LECTURE Dep. of Emergency Medicine, Sung Wook, Song
- 2. WOUND CARE REFERNCES ‣ Tintinalli’s Emergency Medicine, 7th, Section 6: Emergency Wound Management ‣ Rosen’s Emergency Medicine, 8th, Section 4: Soft tissue injuries ‣ Trott AT. Wounds and Lacerations. Elsevier Sciences 2012. ‣ Dealey C. The Care of Wounds. John Wiley & Sons 2012. ‣ Knoop K, Stack L, Storrow A, et al. The Atlas of Emergency Medicine, Third Edition. McGraw Hill Professional 2009. 2
- 3. WOUND CARE CONTENTS 3 1. BACKGROUNDS 2. WOUNDS HEALING 3. WOUND TYPE & CHARACTERISTICS 4. EVALUATION & DOCUMENTATION 5. MANAGEMENT
- 4. WOUND CARE: 1. BACKGROUNDS SKIN STRUCTURE & FUNCTION ▸ Epidermis = Protection ▸ Dermis = nourishment of epidermis ▸ Hypodermis(subcu. tissue) = adipose tissue insulation 4 https://www.youtube.com/watch?feature=player_embedded&v=d-IJhAWrsm0
- 5. WOUND CARE: 1. BACKGROUNDS DEFINITION OF WOUND Discontinuity of the skin, mucous membrane or tissue caused by physical, chemical or biological insult “ 5
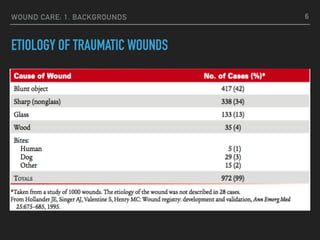
- 6. WOUND CARE: 1. BACKGROUNDS ETIOLOGY OF TRAUMATIC WOUNDS 6
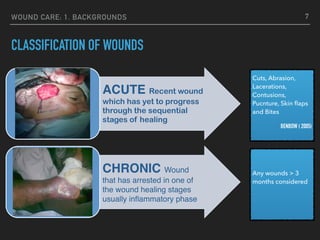
- 7. WOUND CARE: 1. BACKGROUNDS CLASSIFICATION OF WOUNDS 7 ACUTE Recent wound which has yet to progress through the sequential stages of healing CHRONIC Wound that has arrested in one of the wound healing stages usually inflammatory phase Cuts, Abrasion, Lacerations, Contusions, Pucnture, Skin flaps and Bites BENBOW ( 2005) Any wounds > 3 months considered
- 8. WOUND CARE: 1. BACKGROUNDS CLASSIFICATION OF WOUNDS: NEW TREND 8 Acute vs Chronic Wounds SIMPLE WOUND those wounds which are readily managed by local wound care / contraction, direct closure, skin grafting, local tissure rearrangment. COMPLEX WOUND these are large wounds requiring tissue distant from wound site i.e. regional, distal transposition or microvascular composite tissue transfer PROBLEM WOUND Those wounds which fails to achieve closure with the above methods or recurres due to local or systemic causes.
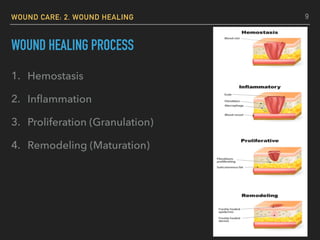
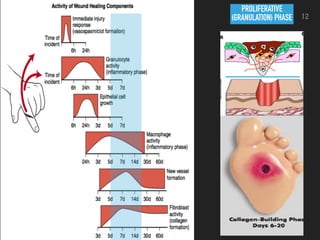
- 9. WOUND CARE: 2. WOUND HEALING WOUND HEALING PROCESS 1. Hemostasis 2. Inflammation 3. Proliferation (Granulation) 4. Remodeling (Maturation) 9
- 10. WOUND CARE: 2. WOUND HEALING WOUND HEALING 1. Hemostasis 2. Inflammation 3. Proliferation (Granulation) 4. Remodeling (Maturation) contraction scarring remodeling 10 KELOID HYPERTROPHIC SCAR
- 14. WOUND CARE: 2. WOUND HEALING NORMAL HEALING PROCESS 14
- 15. WOUND CARE: 2. WOUND HEALING RELATED FACTORS: “DIDN’T HEAL” 15 DIABETES INFECTION DRUGS NUTRITION TISSUE NECROSIS HYPOXIA EXCESSIVE TENSION ON WOUND EDGE ANOTHER WOUND LOW TEMPERATURE
- 16. WOUND CARE: 3. WOUND TYPE & CHARACTERISTICS CLOSED ▸ Contusion: tissue injury w/o breaking of skin ▸ Hematoma: tissue injury that disrupts a blood vessels CONTUSION HEMATOMA 16
- 17. WOUND CARE: 3. WOUND TYPE & CHARACTERISTICS OPENED ▸ Incision ▸ Laceration: traumatic seperation of tissues with clean, smooth edges ▸ Abrasion: traumatic scrapting away of surface layers of skin ▸ Puncture: sharp, pointed object through skin or mucous membrane ▸ Penetrating: variable-sized open wound through skin and underlying tissues ▸ Avulsion: Tearing away of a structure or a part ▸ Ulceration: excavation of skin/underlying tissue from injury or necrosis 17
- 18. WOUND CARE: 3. WOUND TYPE & CHARACTERISTICS ACCORDING TO WOUNDS DEPTH ▸ Superficial: epidermis ▸ Partial Thickness epidermis + dermis ▸ Full Thickness 18
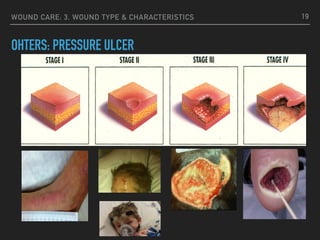
- 19. WOUND CARE: 3. WOUND TYPE & CHARACTERISTICS OHTERS: PRESSURE ULCER 19
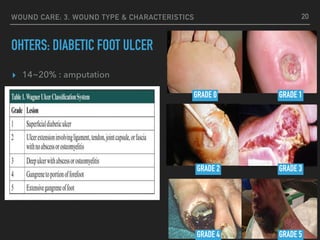
- 20. WOUND CARE: 3. WOUND TYPE & CHARACTERISTICS OHTERS: DIABETIC FOOT ULCER 20 ▸ 14~20% : amputation GRADE 0 GRADE 1 GRADE 2 GRADE 3 GRADE 4 GRADE 5
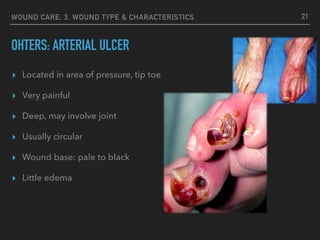
- 21. WOUND CARE: 3. WOUND TYPE & CHARACTERISTICS OHTERS: ARTERIAL ULCER 21 ▸ Located in area of pressure, tip toe ▸ Very painful ▸ Deep, may involve joint ▸ Usually circular ▸ Wound base: pale to black ▸ Little edema
- 22. WOUND CARE: 3. WOUND TYPE & CHARACTERISTICS OHTERS: VENOUS ULCER 22 ▸ Irregular wound edges ▸ Skin scaling ▸ Moderate to heavy exudate ▸ Partial to full thickness ▸ Malleolous region
- 23. WOUND CARE: 3. WOUND TYPE & CHARACTERISTICS OHTERS: SURGICAL WOUND CX. 23 WOUND INFECTION DEHISCENCE
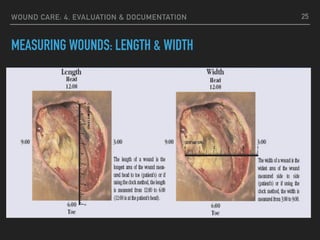
- 24. WOUND CARE: 4. EVALUATION & DOCUMENTATION WOUND DESCRIPTION ▸ Location ▸ Measurements (cm): width x length x depth ▸ Tunneling / undermining ▸ Color of wound bed ▸ Color of exudate (drainage), odors ▸ Condition of surrounding tissue/skin (wound edge) ▸ Sign of infection 24
- 25. WOUND CARE: 4. EVALUATION & DOCUMENTATION MEASURING WOUNDS: LENGTH & WIDTH 25
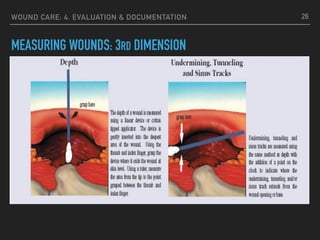
- 26. WOUND CARE: 4. EVALUATION & DOCUMENTATION MEASURING WOUNDS: 3RD DIMENSION 26
- 27. WOUND CARE: 4. EVALUATION & DOCUMENTATION MEASURING WOUNDS 27 3:009:00 12:00 6:00 ▸ Undermining: tissue destruction to underlying intact skin along wound edge ▸ Tunneling/Tracts: a measurable tract from the wound bed ▸ Non-symmetrical: Across longest and widest areas
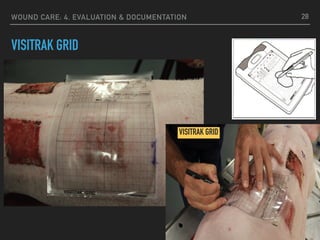
- 28. WOUND CARE: 4. EVALUATION & DOCUMENTATION VISITRAK GRID VISITRAK GRID 28
- 29. WOUND CARE: 4. EVALUATION & DOCUMENTATION STANDARDIZED SERIAL DIGITAL PHOTOGRAPHY 29
- 30. WOUND CARE: 4. EVALUATION & DOCUMENTATION PORTABLE DIGITIZING FOR WOUND MONITORING 30
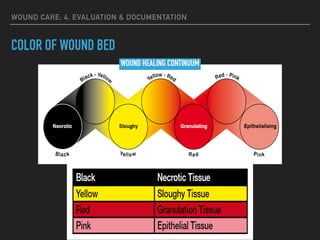
- 31. WOUND CARE: 4. EVALUATION & DOCUMENTATION COLOR OF WOUND BED WOUND HEALING CONTINUUM
- 32. WOUND CARE: 4. EVALUATION & DOCUMENTATION COLOR OF WOUND BED
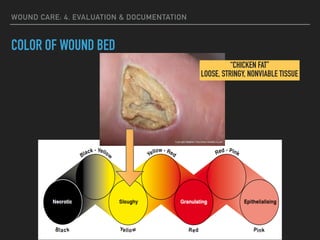
- 33. WOUND CARE: 4. EVALUATION & DOCUMENTATION COLOR OF WOUND BED “CHICKEN FAT” LOOSE, STRINGY, NONVIABLE TISSUE
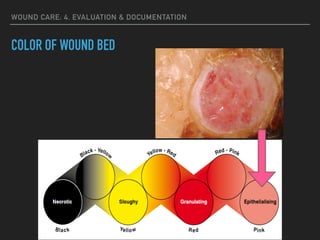
- 34. WOUND CARE: 4. EVALUATION & DOCUMENTATION COLOR OF WOUND BED
- 35. WOUND CARE: 4. EVALUATION & DOCUMENTATION COLOR OF WOUND BED
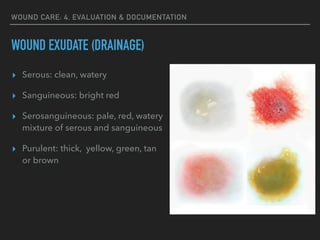
- 36. WOUND CARE: 4. EVALUATION & DOCUMENTATION WOUND EXUDATE (DRAINAGE) ▸ Serous: clean, watery ▸ Sanguineous: bright red ▸ Serosanguineous: pale, red, watery mixture of serous and sanguineous ▸ Purulent: thick, yellow, green, tan or brown
- 37. WOUND CARE: 4. EVALUATION & DOCUMENTATION CONDITION OF SURROUNDING TISSUE/SKIN ▸ Redness ▸ Induration: abnormal firmness of tissue with a definite margin ▸ Callous: firm, thickened area of tissue (DM foot) ▸ Maceration: softening of tissues by soaking in fluids ▸ Denuded: loss of superficial epidermis
- 38. WOUND CARE: 4. EVALUATION & DOCUMENTATION SING OF INFECTION 38 ▸ Increased pain ▸ Copious amounts of exudate ▸ Malodour ▸ Cellulitis ▸ Pyrexia ▸ Inc. size of wound ▸ Pocketing/Abscess formation
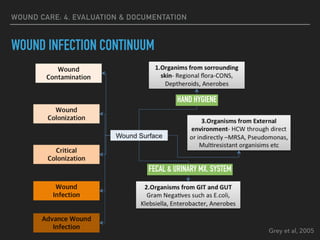
- 39. WOUND CARE: 4. EVALUATION & DOCUMENTATION WOUND INFECTION CONTINUUM
- 40. WOUND CARE: 4. EVALUATION & DOCUMENTATION WOUND INFECTION CONTINUUM Grey et al, 2005 HAND HYGIENE FECAL & URINARY MX. SYSTEM
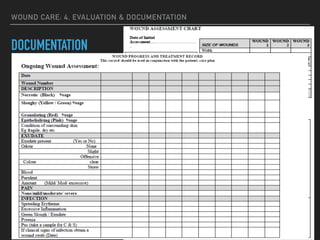
- 41. WOUND CARE: 4. EVALUATION & DOCUMENTATION DOCUMENTATION
- 42. WOUND CARE: 5. MANAGEMENT WOUND CARE PLAN (WCP) DEPENDS ON ▸ Type of wound ▸ Necrotic wound ▸ Sloughy wound ▸ Granulating wound ▸ Epithelialized wound ▸ Infected wound ▸ Mixed wound ▸ Amount & type of Exudate ▸ Critical colonization or infection Wound Care Plan (WCP) Pa#ent Cantered – dealing with person with a chronic wound Holis#c –Total care -Not only wound itself- need to address pts other needs, diseases, and psychosocial wellbeing Inter-disiplinary Needs Par>cipa>on of mul>tude of disciplines 42
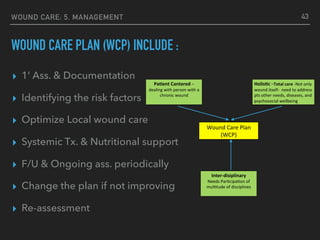
- 43. WOUND CARE: 5. MANAGEMENT WOUND CARE PLAN (WCP) INCLUDE : ▸ 1’ Ass. & Documentation ▸ Identifying the risk factors ▸ Optimize Local wound care ▸ Systemic Tx. & Nutritional support ▸ F/U & Ongoing ass. periodically ▸ Change the plan if not improving ▸ Re-assessment 43 Wound Care Plan (WCP) Pa#ent Cantered – dealing with person with a chronic wound Holis#c –Total care -Not only wound itself- need to address pts other needs, diseases, and psychosocial wellbeing Inter-disiplinary Needs Par>cipa>on of mul>tude of disciplines
- 46. WOUND CARE: 5. MANAGEMENT BASIC WOUND CARE ▸ Cleanse debris from the wound ▸ Possible Debridement ▸ Manage Exudate ▸ Promote Granulation & Epithelialization ▸ Possibly Treat Infections ▸ Minimize Discomfort 46
- 47. WOUND CARE: 5. MANAGEMENT CLEANSE DEBRIS: “THE SOLUTION TO POLLUTION IS DILUTION” ▸ Wound irrigation (N/S): most effective method ▸ Pressure : high (5-70 psi) >> low (0.5-1 psi) 47
- 48. WOUND CARE: 5. MANAGEMENT POSSIBLE DEBRIDEMENT 48 SURGICAL AUTOLYTIC ENZYMATIC BIOLOGICAL MECHANICAL (VERSAJET)
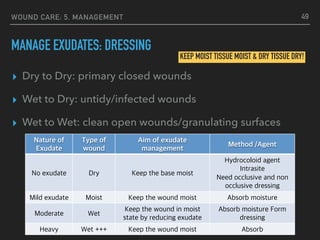
- 49. WOUND CARE: 5. MANAGEMENT MANAGE EXUDATES: DRESSING ▸ Dry to Dry: primary closed wounds ▸ Wet to Dry: untidy/infected wounds ▸ Wet to Wet: clean open wounds/granulating surfaces 49 KEEP MOIST TISSUE MOIST & DRY TISSUE DRY! Nature of Exudate Type of wound Aim of exudate management Method /Agent No exudate Dry Keep the base moist Hydrocoloid agent Intrasite Need occlusive and non occlusive dressing Mild exudate Moist Keep the wound moist Absorb moisture Moderate Wet Keep the wound in moist state by reducing exudate Absorb moisture Form dressing Heavy Wet +++ Keep the wound moist Absorb
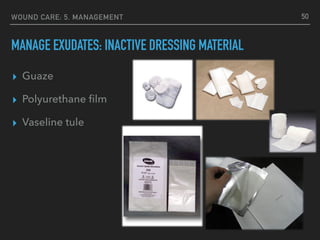
- 50. WOUND CARE: 5. MANAGEMENT MANAGE EXUDATES: INACTIVE DRESSING MATERIAL ▸ Guaze ▸ Polyurethane film ▸ Vaseline tule 50
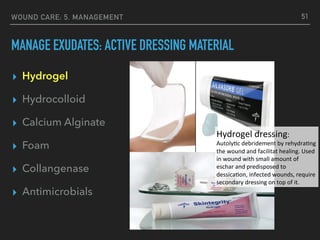
- 51. WOUND CARE: 5. MANAGEMENT MANAGE EXUDATES: ACTIVE DRESSING MATERIAL ▸ Hydrogel ▸ Hydrocolloid ▸ Calcium Alginate ▸ Foam ▸ Collangenase ▸ Antimicrobials 51 Hydrogel dressing: Autoly1c debridement by rehydra1ng the wound and facilitat healing. Used in wound with small amount of eschar and predisposed to dessica1on, infected wounds, require secondary dressing on top of it.
- 52. WOUND CARE: 5. MANAGEMENT MANAGE EXUDATES: ACTIVE DRESSING MATERIAL ▸ Hydrogel ▸ Hydrocolloid ▸ Calcium Alginate ▸ Foam ▸ Collangenase ▸ Antimicrobials 52
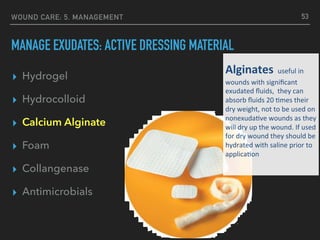
- 53. WOUND CARE: 5. MANAGEMENT MANAGE EXUDATES: ACTIVE DRESSING MATERIAL ▸ Hydrogel ▸ Hydrocolloid ▸ Calcium Alginate ▸ Foam ▸ Collangenase ▸ Antimicrobials 53 Alginates useful in wounds with significant exudated fluids, they can absorb fluids 20 :mes their dry weight, not to be used on nonexuda:ve wounds as they will dry up the wound. If used for dry wound they should be hydrated with saline prior to applica:on
- 54. WOUND CARE: 5. MANAGEMENT MANAGE EXUDATES: ACTIVE DRESSING MATERIAL ▸ Hydrogel ▸ Hydrocolloid ▸ Calcium Alginate ▸ Foam ▸ Collangenase ▸ Antimicrobials 54 Foam dressing Highly absorp.ve and acts like a wick making it useful in highly exuda.ve wounds.
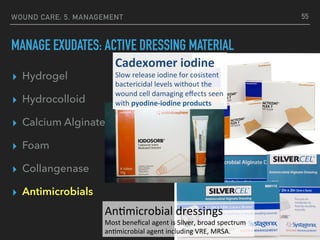
- 55. ▸ Hydrogel ▸ Hydrocolloid ▸ Calcium Alginate ▸ Foam ▸ Collangenase ▸ Antimicrobials WOUND CARE: 5. MANAGEMENT MANAGE EXUDATES: ACTIVE DRESSING MATERIAL 55 Cadexomer iodine Slow release iodine for cosistent bactericidal levels without the wound cell damaging effects seen with pyodine-iodine products An#microbial dressings Most benefical agent is Silver, broad spectrum an#microbial agent including VRE, MRSA.
- 56. WOUND CARE: 5. MANAGEMENT PROMOTE GRANULATION & EPITHELIALIZATION ▸ Granulation enhancers ▸ Minimal dressing changes to reduce disturbances to the granulation ▸ Avoid usage of substances which impede granulation tissues 56
- 57. WOUND CARE: 5. MANAGEMENT TREAT INFECTIONS ▸ Systemic antibiotics ▸ Local antiseptics to the wound 57
- 58. WOUND CARE: 5. MANAGEMENT ADVANCED WOUND CARE ▸ Growth Factors ▸ Bioengineered Tissue ▸ Curative Surgery ▸ Cellular Tissue Products ▸ Negative Pressure wound therapy ▸ Hyperbaric oxygen therapy 58