




























9TH 10TH 11TH 12TH CRANIAL NERVES.pptx
- 1. 9TH 10TH 11TH 12TH CRANIAL NERVES
- 2. GLOSSOPHARYNGEAL NERVE • Upper motor neuron influences on CN IX arise from the primary motor cortex and descend in the corticobulbar tracts to synapse in the rostral portion of the nucleus ambiguus in the dorsolateral medulla. The cortical innervation is bilateral. The cells in the nucleus ambiguus are branchiomotor and innervate muscles derived from the third, fourth, and sixth branchial arches. The nerve emerges from the medulla as three to six rootlets in the groove between the inferior olive and the inferior cerebellar peduncle, between and in line with the emerging fibers of CN VII above and CN X. These rootlets unite to form a single nerve, which leaves the skull through the jugular foramen.
- 5. • CN IX exits the skull through the jugular foramen, lateral and anterior to CNs X and XI within a separate dural sheath. After leaving the skull, CN IX enters the carotid sheath, descends between the internal jugular vein and internal carotid artery, dips beneath the styloid process, and then passes between the internal and external carotid arteries. It curves forward, forming an arch on the side of the neck to reach the lateral pharyngeal wall, and then disappears under the hyoglossus muscle to divide into its terminal branches.
- 6. • Two ganglia lie on the nerve just caudal to the jugular foramen: the superior (jugular) and inferior (petrosal) glossopharyngeal ganglia. The superior glossopharyngeal ganglion is small, is inconstant, has no branches, and is often fused with the inferior ganglion.
- 8. • CN IX has six terminal branches: (a) the tympanic nerve (Jacobson’s nerve), (b) carotid, (c) pharyngeal, (d) muscular, (e) tonsillar, and (f) lingual branches
- 10. EXAMINATION OF 9TH NERVE • The pharyngeal reflex is the more active. • The reflex occurs with touching the base of the tongue or posterior pharyngeal wall. • The afferent limb of the reflex is mediated by CN IX and the efferent limb through CNs IX and X. The reflex center is in the medulla. The motor response is constriction and elevation of the oropharynx. This causes the midline raphe of the palate and the uvula to elevate and the pharyngeal constrictors to contract. The activity on the two sides is compared. There are three motor components: elevation of the soft palate to seal off the nasopharynx, closure of the glottis to protect the airway, and constriction of the pharynx to prevent entry of the substance
- 11. DISORDERS OF FUNCTION • Nuclear and infranuclear processes that may affect CN IX include intramedullary and extramedullary neoplasms and other mass lesions (e.g., glomus jugulare tumor), trauma (e.g., basilar skull fracture or surgical dissection), motor neuron disease, syringobulbia, retropharyngeal abscess, demyelinating disease, birth injury, and brainstem ischemia
- 12. • GLOSSOPHARYNGEAL NEURALGIA ALSO CALLED AS TIC DOULOUREUX OF NINTH NERVE – CAUSES AND AGGREVATING FACTORS • JACOBSONS NEURALGIA
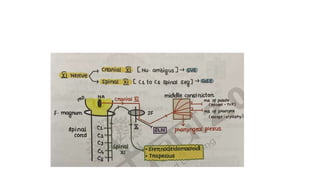
- 13. VAGUS NERVE • The vagus emerges from the medulla as a series of rootlets just below those of the glossopharyngeal. CN X leaves the skull through the jugular foramen in the same neural sheath as the cranial root of CN XI and behind CN IX. In the jugular foramen, the nerve lies close to the jugular bulb, a dilatation of the internal jugular vein that houses the glomus jugulare (tympanic body). The glomus jugulare has functions similar to the carotid body. CN X descends the neck in the carotid sheath, lying between the carotid artery and internal jugular vein to the upper border of the thyroid cartilage and then between the vein and common carotid to the base of the neck.
- 15. • Branches leave in the jugular foramen to supply the meninges and ear; other branches leave distal to the foramen to supply the pharynx and larynx. The major portion of the nerve enters the thorax. The vagus has two sensory ganglia. The superior (jugular) vagal ganglion is located in the jugular fossa of the temporal bone; the inferior (nodose) ganglion is located just distal to the jugular foramen. There are 10 major terminal branches that arise at different levels: (a) meningeal, (b) auricular, (c) pharyngeal, (d) carotid, (e) superior laryngeal, (f) recurrent laryngeal, (g) cardiac, (h) esophageal, (i) pulmonary, and (j) gastrointestinal.
- 18. • A unilateral vagal lesion causes weakness of the soft palate, pharynx, and larynx. Acute lesions may produce difficulty swallowing both liquids and solids and hoarseness or a nasal quality to the voice. The only definite sensory change is anesthesia of the larynx because of involvement of the superior laryngeal nerve. The gag reflex is absent on the involved side. Autonomic reflexes (vomiting, coughing, and sneezing) are not usually affected. Tachycardia and loss of the oculocardiac reflex on the involved side may occur.
- 20. • . Bilateral complete vagal paralysis is incompatible with life. It causes complete paralysis of the palate, pharynx, and larynx, with marked dysphagia and dysarthria; tachycardia; slow, irregular, respiration; vomiting; and gastrointestinal atonia. Lesions of individual vagal branches are rare except for involvement of the recurrent laryngeal nerve
- 22. REFLEXES OF 10TH NERVE • OCULOCARDIAC REFLEX • VOMITING REFLEX • CAROTID SINUS REFLEX • VASO VAGAL ATTACK
- 24. • CN XI emerges from the skull posteromedial to the styloid process and then descends in the neck near the internal jugular vein, behind the digastric and stylohyoid muscles, to enter the deep surface of the upper part of the SCM muscle. It passes through the SCM, sending filaments to it, and then emerges at its posterior border near the midpoint, coursing near the great auricular nerve. CN XI then runs obliquely across the posterior triangle of the neck on the surface of the levator scapula muscle, superficially and in close proximity to the lymph nodes of the posterior cervical triangle. About three fingerbreadths above the clavicle, the nerve enters the deep surface of the anterior border of the upper trapezius muscle.
- 27. HYPOGLOSSAL NERVE • The hypoglossal nerve (CN XII) is a purely motor nerve, supplying the tongue. Its cells of origin are in the hypoglossal nuclei, which are upward extensions of the anterior gray columns of the spinal cord; they consist of large, multipolar cells, similar to the anterior horn motoneurons. The paired nuclei extend almost the entire length of the medulla just beneath the floor of the fourth ventricle, close to the midline • The hypoglossal fibers gather into two bundles, which perforate the dura mater separately, pass through the hypoglossal canal, and then unite. The nerve descends through the neck to the level of the angle of the mandible and then passes forward under the tongue (hence its name) to supply its extrinsic and intrinsic muscles
- 30. • ALL MUSCLES OF PALATE • ALL MUSCLES OF PHARYNX • ALL MUSCLES OF LARYNX • ALL MUSCLES OF TONGUE
- 31. •THANK YOU