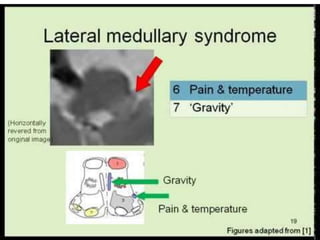
Lateral medullary syndrome {Wallenberg Syndrome}
•Download as PPTX, PDF•
59 likes•22,066 views

Wallenberg syndrome, also known as lateral medullary infarction, is caused by occlusion of the posterior inferior cerebellar artery, which supplies blood to the lateral medulla. This leads to vertigo, abnormal eye movements, Horner's syndrome on one side, ataxia of the limb on the same side, and dissociated sensory loss. The condition is usually due to atherosclerosis but can also result from traumatic vertebral artery dissection. MRI and MRA are used to diagnose the infraction and rule out arterial dissection.
Lateral medullary syndrome {Wallenberg Syndrome}
- 1. Lateral Medullary Syndrome Wallenberg syndrome Prof. Ahmed M Badheeb, MD. Professor Of Oncology /Internal Med.
- 2. Wallenberg syndrome • or lateral medullary infarction, is associated with the acute onset of vertigo and disequilibrium. • The blood supply to the lateral medulla is the posterior inferior cerebellar artery.
- 3. PATHOPHYSIOLOGY • Most patients with Wallenberg's syndrome have an occlusion of the ipsilateral vertebral artery that gives rise to the posterior inferior cerebellar artery .
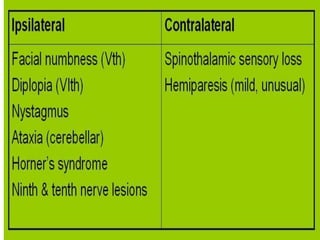
- 4. The clinical presentation, • Vertigo • abnormal eye movements • an ipsilateral Horner syndrome • ipsilateral limb ataxia • dissociated sensory loss (loss of pain and temperature sensation on the ipsilateral face and contralateral trunk with preserved vibration and position sense). • Hoarseness and dysphagia are often present.
- 5. Etiology • Wallenberg's syndrome usually occurs as a result of atherosclerotic or lipohyalinotic arterial occlusion, but it is also a common presentation for traumatic vertebral artery dissection. • A history of neck injury or neck pain suggests the latter.
- 6. The diagnosis • is established definitively with MRI. • MRA of the head and neck should be performed as well to rule out arterial dissection. • Patients usually recover their equilibrium after several months.