Tension pneumothorax
•Download as PPTX, PDF•
5 likes•9,171 views

there is the introduction part of the torso trauma, check out my next ppts for further more about torso trauma. contents are in following order... introduction mechanism of injury junctional zones of torso tension pneumothorax cardiac temponade massive hemothorax etc. check out all slides










Tension pneumothorax
- 1. Presented by : BHAVIKA SAHU Roll No. : 25 MBBS FINAL YEAR II DEPARTMENT OF SURGERY Lt.BRKM GMC JDP
- 2. Introduction Incidence Etiology Pathophysiology Clinical features -symptoms -signs Management Complications Differential diagnosis Bibliography
- 3. Pneumothorax is the presence of air between the layers of pleura. It is the most common cause of respiratory insufficiency following chest trauma. Pneumothorax can be – - closed(or simple) - open - tension
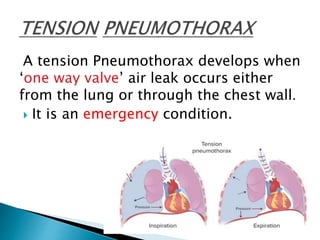
- 5. A tension Pneumothorax develops when ‘one way valve’ air leak occurs either from the lung or through the chest wall. It is an emergency condition.
- 6. Patients with trauma tend to have an associated pneumothorax or tension pneumothorax 20% of the time. In cases of severe chest trauma, there is an associated pneumothorax 50% of the time. The incidence of traumatic pneumothorax depends on the size and mechanism of injury.
- 7. TRAUMATIC Penetrating chest trauma Blunt force trauma Iatrogenic lung injury NONTRAUMATIC Mechanical positive pressure ventilation
- 8. PATHOPHSIOLOGY Injury to the lung Valvular air leak Lung collapse Mediastinal shift to opposite side
- 9. Increased intrapleural pressure Decreased venous return Decreased ventilation Hypoxia and cardiac aarest
- 10. SYMPTOMS - ACUTE CHEST PAIN - SHORTNESS OF BREATH - RESTLESSNESS - ANXIETY
- 11. TACHYPNOEA CYANOSIS TACHYCARDIA JUGULAR VENOUS DISTENSION HYPOTENSION
- 12. INSPECTION – Decreased chest movements PALPATION – Mediastinal and trachea shifts to the Contralateral side. PERCUSSION – Hyperresonant note. AUSCULTATION- Absent breath sounds.
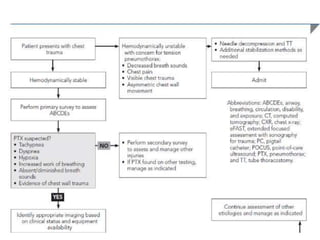
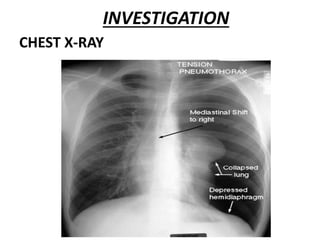
- 13. MANAGEMENT • TENSION PNEUMOTHORAX Is a CLINICAL DIAGNOSIS. • Management should not Wait for Image confirmation. • If the patient is hemodynamically unstable, then immediate needle decompression must be performed without delay followed by ICD insertion and connected to underwater seal.
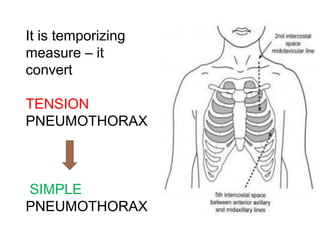
- 16. 14 -16 gauge needle is inserted through the chest wall . In 2nd intercostal space–midclavicular line In 5th intercostal space- just anterior to Mid axillary line
- 17. It is temporizing measure – it convert TENSION PNEUMOTHORAX SIMPLE PNEUMOTHORAX
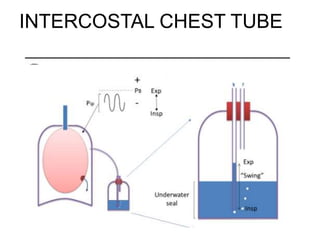
- 21. Chest tubes are always connected to an underwater seal bag to prevent air from re – entering . Functioning of chest tube is assessed by movement of column of fluid in the water bag . Position of the chest tube checked by taking chest X-ray
- 24. RESPIRATORY FAILURE RESPIRATORY ARREST CARDIAC ARREST SUBCUTANEOUS EMPHYSEMA PNEUMOPERICARDIUM PNEUMOPERITONEUM
- 25. PROCEDURE COMPLICATIONS Fistula formation Infections Bleeding Intercostal nerve injury
- 26. CARDIAC TAMPONADE HEMOTHORAX PULMONARY EMBOLISM MYOCARDIAL INFARCTION ACUTE AORTIC DISSECTION RIB FRACTURE COSTOCHONDRITIS DIAPHRAGMATIC INJURY
- 27. •BAILEY AND LOVE •SRB’S MANUAL OF SURGERY
- 28. THANK YOU